

Public Charge Proposed Rule Threatens Immigrant Health Care
The Trump Administration’s proposed rule that changes how the Department of Homeland Security determines whether a person is likely to become a “public charge” has generated a large volume of response. During the public comment period that ended December 10, over 200,000 comments were generated on the proposed rule to the “Inadmissibility in Pubic Charge Grounds.”
Alex Shekhdar, vice president of federal and state policy at Medicaid Health Plans of America, expressed that the high volume of response stands as testament for the large and “vitriol” impact the proposed changes will have on people and the coming implications for health care delivery and cost.
“If these changes go into effect, there will be a huge churn effect on enrollment,” Mr Shekhdar said, referring to people going on and off plans. “Immigrant families will be in fear that availing themselves of different public programs will prejudice their immigration status or that of their family members.”
As to the delivery of care, the proposed changes will promote what Mr Shekhdar referred to as under-the-table health care. “By definition, this is the antithesis of coordinated care,” he said. “So if people are going to under the table health care, they are not leveraging the purpose of the managed care system, which is coordinated care to improve health care outcomes.”
Public Charge and Proposed Changes
Under the current statute, potential immigrants seeking permanent admission to the United States, nonimmigrants seeking temporary admission to the United States, and most foreign nationals seeking visas to the United States must pass a test that shows that they will not “likely become a public charge (LCP).” Through the LCP test, they have to be able to show that after receiving a green card or other visa they will not in the future likely need to be primarily dependent on forms of public cash assistance for income maintenance (eg, supplemental security income, temporary assistance for needy families, or general assistance) and will not require long-term care assistance (eg, nursing home.)
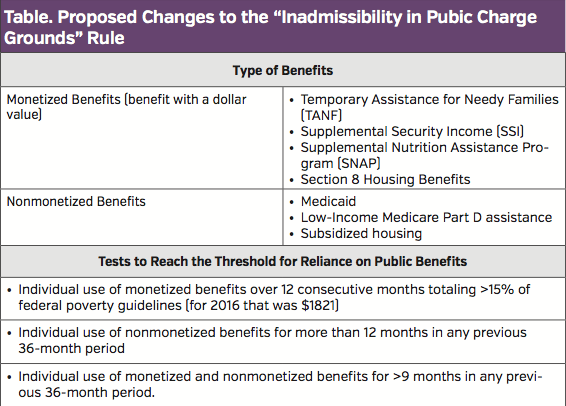
Under the new proposed changes to the rule, the Department of Homeland Security expands the definition of “public charge” as someone who in the future is likely to need supplementary forms of public assistance not covered under the original rule. The table lists the types of new supplementary forms of assistance as well as tests based on these categories to reach the threshold for reliance on public benefits.
Although there may be exemptions in the proposed rule, such as SNAP benefits for children, Gerard A. Vitti, president & CEO of Health care Financial, Inc. of Quincy, MA., a firm specializing in enrolling the uninsured into health programs, emphasized that there is a lot of uncertainty about what these measures mean.
“Essentially, if you use any public dollars it works against you when applying for citizen status,” Mr Vitti said. “Folks today can get coverage for Medicaid, whereas under the proposed public charge they would fail to get health services that use Medicaid dollars as that will count against them in their application for new citizenship.”
Chilling Effect
Such changes in the proposed public charge rule will first and foremost have a chilling effect on immigrants and others who are applying for permanent or temporary admission to the United States. “It becomes a Sophie’s Choice between accessing health care and other social services and potentially giving up the dream of getting a certain immigration status,” said Mr Shekhdar.
Although the government estimates that changes to the rule will affect only about 383,000 people who will need to take the test annually, others estimate the numbers affected as much higher. Some projections estimate about 900,000 immigrants and 176,00 million nonimmigrants affected each year. Others expect the most affected group by the new proposed rule will be immigrants seeking green cards to come the United States to be with their families, a group that typically have lower income, less education, and are older and more likely to be considered a public charge.
Mr Vitti agreed that the estimated number of people is likely to be far more than projected. “I don’t have a good estimate, but I can tell you what happens whenever you do Medicaid expansion,” he said. “[Officials] under-project the number of people who sign up, meaning that there are more people in the program than they expect.”
For Mr Vitti, the proposed changes to the rule go against the grain of what is happening with Medicaid expansion. “This past election was in part a referendum on expanding Medicaid, even in the reddest of states, and [these proposed changes to the rule are] a push back in the wrong direction of contracting Medicaid enrollment,” he said.
That contraction, he emphasized, is detrimental to the health status of people who no longer will have coverage. “When you contract coverage, you end up with more sick people.”
This in turn leads to the second big problem with the proposed rule, the adverse effect on the health care system.
Wrong Direction: Health Care Delivery
Saying that the proposed public charge rule is bad for the health care system, Mr Vitti emphasized two main interrelated effects that will drive up cost and decrease health status. First is the detrimental effect on health plans as people go on and off plans (churn) and the subsequent use of higher cost care.
“[The proposed rule] will hurt current health plans as folks come on and off the programs,” he said. “And this is bad for the health care system as hospitals will see more emergency room usage and will see more unpaid bills that will hurt their support of serving the poor.”
Mr Shekhdar agreed. “The downstream impact of the churning impact on enrollment of people going on and off the rolls and not availing themselves of health benefits that they may be eligible for will divert them to other sources of care, such as hospitals and emergency rooms, where they might not disclose their immigration status,” he said.
In a letter to the Department of Homeland Security sent during the public comment period, Francis Rienzo, interim CEO, Medicaid Health Plans of America, succinctly laid out what this shift from lower-cost preventive and managed care to high-cost urgent care under the proposed rule would be in terms of cost.
“A recent analysis estimated that $17 billion in annual hospital payments (based on 2016 data) related to care for Medicaid and CHIP enrollees would be at risk as a result of the policies under the proposed rule,” stated Mr Rienzo.
Managed care, he emphasized, would be weakened and undermined. In particular, he pointed out how the proposed rule would undermine Medicaid managed care plans focus on managing cost through ensuring use of appropriate services and coordinated care.
One area of concern to Mr Vitti is the impact the proposed rule would have on efforts to address the opioid crisis. “Plans using case management see a lot of opioid addiction,” he said. “You can’t manage opioid addiction for folks under this proposed public charge. That is giving them a death sentence.”
Immigration Issue
Although no timeline is set for when the final rule may come out, Mr Shekhdar thinks it may be sooner rather than later given the current focus on immigration. “The policy impetus behind [the proposed public charge], which is immigration, will have a negative impact on something that should be kept separate from health care,” he said.
“This is part of the antiimmigration issue,” Mr Vitti agreed. “The Administration has aligned with Trump to push out undocumented immigrants but also to reduce enrollment of people who get into the country legally to get citizenship.”
Regardless of the impetus behind the proposed public charge, if it does go into effect, managed care plans will need to be ready. “Much like community engagement, given our plans have a direct interface with a Medicaid beneficiary, whatever comes out will require certain changes to operational processes to accommodate this new policy,” said Mr Shekhdar.


