

Perioperative Considerations for Minimally Invasive Foot and Ankle Surgery
Percutaneous and minimally invasive surgery (MIS) techniques within the arena of foot and ankle surgery appear to be gaining popularity, among both orthopedic and podiatric subspecialists, and within the United States and internationally. MIS surgical techniques, in my observation, appear to be a common ground being found by global foot and ankle surgeons, with many national and international courses now available. Improvement in technologies surrounding implants, fixation systems, and preoperative evaluations with advanced tools such as weight-bearing computed tomography (CT), patient-specific instrumentation (PSI), and 3D printing have allowed surgeons to refine and successfully employ MIS techniques.
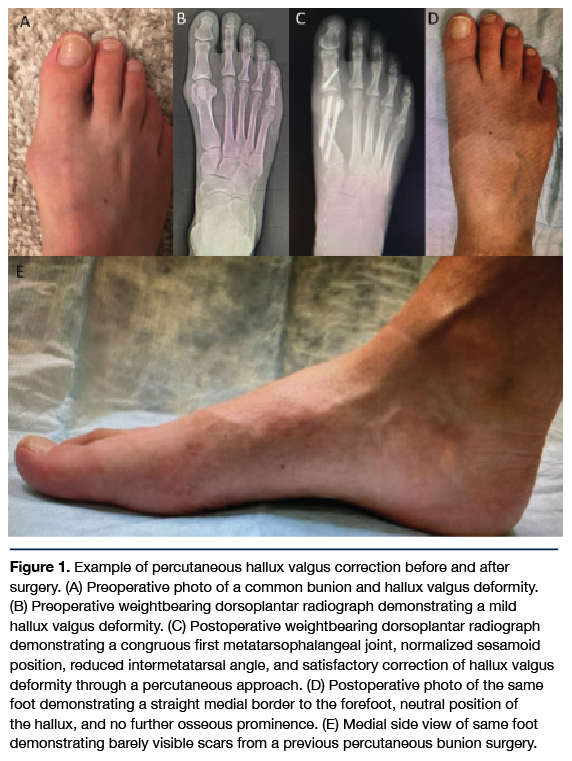
A body of literature continues to grow and evolve pertaining to the MIS arena, which demonstrates that these techniques can be equal in safety and efficacy compared to their open equivalents for addressing common foot and ankle pathologies.1-3 A caveat must be inserted at this time, as these techniques carry a steep learning curve,4-5 which must be mastered prior to these benefits being realized by the patients and surgeons employing them. Nevertheless, MIS approaches offer additional benefits to patients and surgeons such as smaller, cosmetically pleasing scars, faster recovery, reduced postoperative pain, decreased postoperative joint stiffness, immediate weight-bearing, and decreased operative time (Figure 1).1–5 A retrospective review published in 2022 involving 274 feet that underwent percutaneous chevron-Akin osteotomies for hallux valgus correction demonstrated high patient satisfaction rates and excellent radiographic correction when comparing preoperative versus postoperative intermetatarsal and hallux valgus angles, but most impressively noted a mean postoperative narcotic pain pill consumption of 2.2 (5 mg) oxycodone pills.6
Understanding Key Definitions and Applications
For purposes of this article, when discussing MIS, we will assume this includes percutaneous techniques. However, it is important to set some definitions, as not all foot and ankle procedures fall into these categories. Additionally, there may be procedures that are commercially marketed as MIS, but may fall short of the true definition. In my experience, “percutaneous” foot and ankle surgery refers to making the smallest possible incision where the surgeon has no direct visualization of the anatomical structure operated upon. This often relies upon tactile sensation and fluoroscopy to accomplish the goals of the procedure. In my experience, “MIS” refers to making the smallest possible incision that still permits direct visualization of the anatomical structure being operated upon. This may still require use of tactile sensation and fluoroscopy, although typically less than percutaneous approaches. Other terms referring to varying approaches that one may encounter include “mini-open,” “arthroscopic-assisted,” and traditional “open.” However, these types of procedures do not fall under MIS and are beyond the scope of this article.
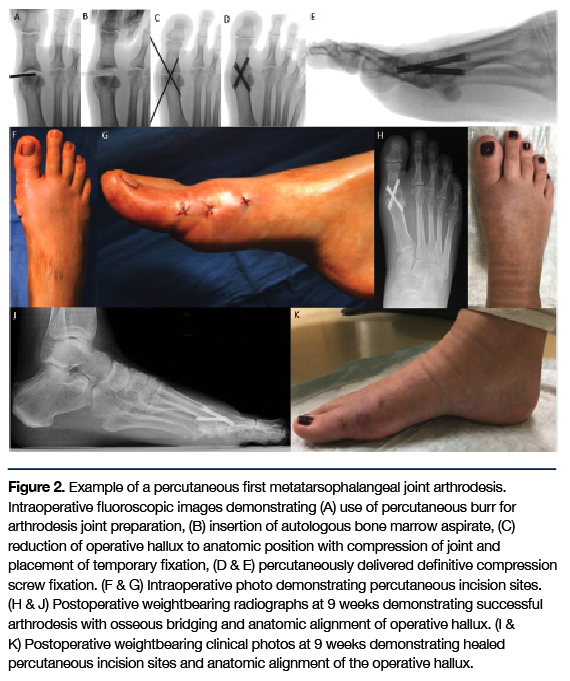
When analyzing MIS foot and ankle surgical procedures further, there exists a myriad of common procedures I now see regularly approached via MIS technique. These include surgical correction of hallux valgus, hallux rigidus, hammertoe deformities, and tailor’s bunion deformities, to name a few. Additionally, specific MIS procedures have been refined to address various foot and ankle pathology by means of MIS osteotomies or arthrodesis. Examples include distal minimally invasive metatarsal osteotomies (DMMO), percutaneous calcaneal osteotomies, and MIS arthrodesis of many ankle and foot joints. For example, arthrodesis of the first metatarsophalangeal joint can be accomplished through a percutaneous approach and offers reproducible outcomes with high patient satisfaction, but also carries the aforementioned benefits of MIS7-11(Figure 2). Even highly complex pathophysiological conditions such as Charcot are being addressed more and more through a MIS approach.12
Industry involvement has also fueled the advancement of MIS techniques and is a driving force in attempting to lower the learning curve through improved technologies and fixation systems resulting in more reproducible outcomes. When combining this with the aforementioned MIS patient benefits, growing surgeon interest, and evidence-based literature highlighting superior outcomes over open approaches, this author sees MIS having a large influence on shaping foot and ankle care pathways in the future. The intention of this article is not to delve into specific foot and ankle MIS procedures, as this would be extensive and involve a volume of information beyond the capacity of this article. Moreover, the purpose of this article is to review perioperative topics and considerations as they relate to foot and ankle MIS.
MIS Indications and Contraindications
Determining which patients are appropriate candidates for foot or ankle surgery can be challenging. Most of the indications and contraindications that apply for open surgical procedures also apply for MIS foot and ankle procedures. MIS can be employed for primary or revision surgeries. Early on in a surgeon’s learning curve, MIS may be best applied for pathologies of more mild-to-moderate complexity. As one overcomes the learning curve and masters MIS techniques, one may choose to expand the potential application. This may include circumstances in which a surgeon previously would not have considered operating on a patient due to being a “poor surgical candidate.” In this scenario, one may determine that the patient’s risks are no longer greater than the potential benefit, and the surgeon can at least comfortably offer the patient a MIS surgical approach over no surgery at all. Having MIS techniques in a surgeon’s toolbox may then likely result in a larger potential surgical population.
Before scheduling elective foot and ankle MIS procedures, patients should have failed prior conservative treatment modalities depending upon the specific pathology being treated, including but not limited to: over-the-counter oral and/or topical analgesics/anti-inflammatories, shoe gear modifications, padding/strapping, functional bracing, orthotic management, injections (corticosteroid, platelet-rich plasma), physical therapy, and immobilization. Absolute contraindications may include active osteomyelitis, peripheral vascular disease, and severe osteoporosis. A history of previous foot and ankle surgery is not necessarily a contraindication to MIS approaches, and in some situations may be of significant benefit. For example, patients who have severe scarring or a hostile soft tissue envelope from prior surgery may benefit from an MIS approach to obviate additional scarring and decrease risks of postoperative wound healing complications.
Perioperative Pearls to Consider
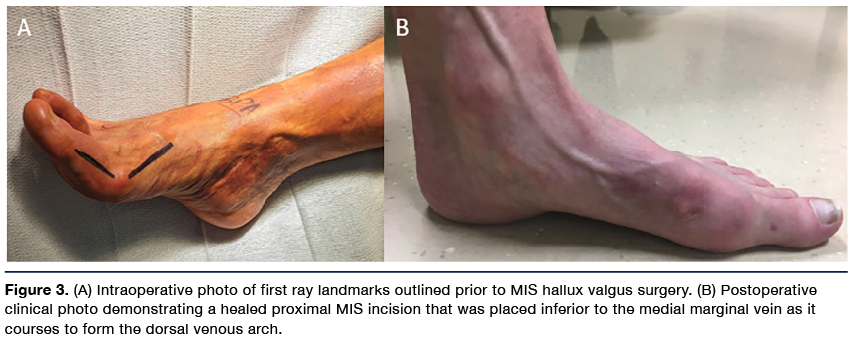
When performing foot and ankle surgery through a MIS approach, there are certain pearls to keep in mind. First, draw anatomical landmarks on the integument of the operative lower extremity. Because the procedures are carried out through either percutaneous or minimal incisions, a surgeon will not have the same visualization one is typically accustomed to through an open approach. Osseous and joint landmarks can typically be identified through palpation, or one can utilize intraoperative fluoroscopy to identify these structures, which can then be outlined. These reference points simplify and facilitate proper placement of fixation for osteotomies and arthrodeses later in the operation, which commonly involve percutaneously delivered implants. Moreover, incision placement should take place in known foot and ankle anatomical “safe zones” whenever feasible. Various venous and nervous structures are readily visible on gross examination and should be avoided when possible (Figure 3). A handheld Doppler can also be utilized to map out the course of arterial inflow so that the surgeon can circumvent and protect these structures.
Additionally, foot and ankle surgeons may find benefit from utilization of preoperative templates, similar to their use in traditional open surgery. On preoperative imaging, one should consider measuring any potential implant or fixation lengths. This is ideally done on a preoperative computerized tomography (CT) scan if available, but this author recognizes that not all foot and ankle pathology will require preoperative CT evaluation. Preoperative measurements serve as a “double check” when it comes time to obtain intraoperative measurements for MIS fixation (Figure 4).
Depending upon the MIS procedure, there are also Food and Drug Administration (FDA)–approved external jig systems that can aid in osteotomies, joint preparation for arthrodesis, deformity correction, and delivery of internal fixation. These systems exist commonly for percutaneous and MIS surgical correction of hallux valgus deformities, and more will likely be developed in the future focused on other foot and ankle pathologies. External jigs may improve surgeon accuracy for addressing pathology, aiding deformity correction, and facilitating accurate placement of internal fixation. Furthermore, jigs may help to lower the learning curve and facilitate reproducible outcomes, especially for surgeons who are just starting an MIS journey. Finally, there may even be a greater role for utilizing preoperative weight-bearing CT scans, intraoperative CT, or even patient-specific instrumentation (PSI), which would be another available level of perioperative support.
Considering Anesthesia and Perioperative Patient Comorbidities
Similar to traditional open foot and ankle surgeries, appropriate medical clearance and screening for relevant comorbidities should be obtained preoperatively as indicated. This aids in solidifying a thoughtful surgical treatment plan, but also helps determine the appropriate type of anesthesia for the patient’s MIS surgery. The majority of this author’s MIS foot and ankle procedures are performed under general anesthesia; however, there are many MIS surgeries easily performable under monitored anesthesia care with supplemental regional local anesthetic blocks, or spinal anesthesia.
Similar to open surgery, it is wise to vet patients for modifiable risk factors that may influence their potential healing of soft tissue and osseous procedures, or place them at risk for perioperative complications. Tobacco cessation should be discussed and encouraged, and quitting resources should be offered to patients considering elective MIS foot and ankle surgery. Furthermore, the potential risks of continuing tobacco use through the perioperative period should be reviewed with the patient if they choose not to relinquish. A multidisciplinary approach is also wise for patients on glucocorticoids or certain rheumatologic medications that may influence postoperative healing. Involving a patient’s primary care physician, rheumatologist, endocrinologist, and anesthesia is helpful when potentially holding such medications in the perioperative period to safely mitigate perioperative risks.
Intraoperative Positioning and Equipment Set-up
After appropriate evaluation and vetting as a candidate for MIS foot and/or ankle surgery, patient positioning is the first, and often most indispensable, initial step towards successful outcomes. In the author’s experience, a minimum of the distal third, and up to the distal half, of the operative lower extremity should hang off the end of the operating table. It is the author’s preference to have the patient’s anatomy from mid-calf to operative foot hanging off the operative table for MIS foot and ankle procedures.
It is up to the surgeon’s preference whether to use an intraoperative tourniquet. Some surgeons do not utilize a tourniquet, and mild bleeding offers an additional benefit of cooling the sterile burrs utilized for MIS procedures. For surgeons employing a tourniquet, the use of chilled saline can also offer a similar effect intraoperatively.13
The patient is also placed in mild head-down Trendelenberg positioning, as a tourniquet is often avoided. The nonoperative lower extremity is padded and placed on an extra arm board to facilitate placement away from the operative field (Figure 5). This specific positioning allows fluid unobstructed use of surgical instrumentation. Additionally, it permits optimal positioning of intraoperative fluoroscopy with manipulation ability in multiple planes throughout the duration of the procedure. For a right hand–dominant surgeon, he or she sits or stands on the left side of the patient’s operative lower extremity. This fluoroscopy unit should be positioned at, and enter the operative field from, the right side of the operative lower extremity. The operative lower extremity is scrubbed, prepped, and draped following standard aseptic technique, again assuring unobstructed access to the operative foot and ankle.
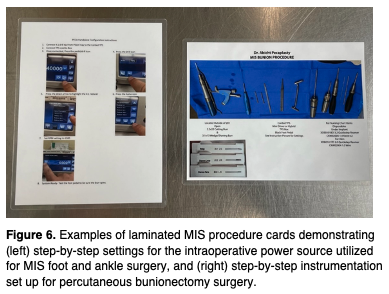
The MIS learning curve for foot and ankle surgeons has been documented in the literature.4-5 However, there may also exist a learning curve for personnel supporting the surgeon, as most operative scrub technicians and nurses are most familiar with traditional open surgeries. It can be helpful to utilize laminated surgical cards for assistants to reference prior and during MIS surgeries (Figure 6). These cards can outline specific power settings, name instrumentation, and afford step-by-step approaches for foot and ankle MIS procedures. Operating in the pandemic and post-pandemic timeframe has created many challenges relating to consistent staffing, variable intraoperative industry representation, and has even hindered standard room turnover or sterilization protocols. Thus, such reference guides are invaluable and help bring unfamiliar support staff up-to-speed rapidly.
Using Intraoperative Fluoroscopy
MIS foot and ankle procedures require the use of either tactile sensation and/or intraoperative fluoroscopy to successfully accomplish the goals of a given procedure. In the author’s observation, this inherently results in increased utilization of intraoperative fluoroscopy. As such, surgeons should take precautions to protect their patients and themselves during these procedures. A mini c-arm can be utilized for any MIS foot or ankle surgery. This obviates the need for a larger c-arm, which carries increased levels of radiation exposure for the patient, surgeon, and surgical staff. Additionally, this author routinely employs a lead apron and lead thyroid shield during MIS surgery. Non-sterile lead gloves should be employed when a surgeon has his or her hands within the radiation field when preoperatively stressing the operative foot and ankle. Intraoperative radiation-attenuating sterile gloves should also be considered for MIS surgeons, and are already utilized in other subspecialties such as interventional radiology. Similarly, leaded antiradiation eyewear is available to mitigate the secondary effects of intraoperative fluoroscopy usage for MIS foot and ankle surgery.
MIS Procedure Finalization and Postoperative Course
At the culmination of a foot and ankle MIS surgery, this author typically provides a long-acting local anesthetic ankle ring-block (with epinephrine if indicated) for postoperative analgesia to the operative lower extremity. Percutaneous and MIS incisions may be closed via various methods. This could include nonabsorbable suture to approximate skin margins; alternatively, an absorbable monofilament can be utilized to close the subcuticular layer with wound closure surgical tape strips applied to the external skin. If percutaneous or MIS incision sites experience minor iatrogenic complications, such as thermal injury, torn or shredded skin edges, or pressure injury, they should be addressed prior to incision site closure. If possible with the damaged skin or wound site, one should undertake excision to prevent future incision site delayed healing, dehiscence, or potential postoperative wound complications.
Small incisions associated with foot and ankle MIS procedures are not only cosmetically pleasing to patients, but also avoid the significant dissection and soft tissue stripping witnessed in traditional open surgery, which can also result in increased postoperative swelling and pain. One of the major benefits of MIS foot and ankle surgery is the decreased postoperative pain level compared to the same open procedures, which has resulted in less postoperative narcotic pain medication consumption by patients.6
Postoperative bandaging is a crucial adjunct to many MIS foot and ankle procedures. A well-padded foot and ankle compression bandage applied to the operative lower extremity can control postoperative edema (Figure 7). If a patient has significant baseline lower extremity edema, for example from chronic venous insufficiency or lymphedema, then the postoperative dressing can be carried up to the knee. This can prevent the dressing from cutting into the ankle or distal leg or causing discomfort along with mechanically encouraging fluid into the popliteal lymph nodes. Depending upon the type of procedure, strapping/splinting/taping of certain digits is commonly utilized to maintain and augment deformity correction.
Another benefit for most MIS foot and ankle surgeries includes immediate weight-bearing on the patient’s postoperative foot. Common procedures in which this applies include (but is not limited to): percutaneous or MIS hallux valgus surgery (Figure 8), MIS tailor’s bunion surgery, MIS hammertoe procedures, percutaneous cheilectomy, DMMO, percutaneous first metatarsophalangeal joint arthrodesis (Figure 2), MIS Lapidus procedures, and percutaneous Zadek-type calcaneal osteotomies. It is this author’s preference to permit immediate weight-bearing in a flat rigid postoperative shoe with the patient being instructed to avoid a propulsive gait. Patients are seen between 2 and 3 weeks postoperatively for suture removal, at which time they are instructed to start passive and active range of motion exercises (dependent upon the procedure performed). For patients that underwent an MIS procedure that permits immediate weight-bearing, this author permits return to work for light duty (desk work, seated position) once incision sites are healed and sutures removed. It is still recommended that patients utilize elevation, intermittent ice therapy, compression garments, and activity modifications/restrictions to aid in limiting postoperative edema and discomfort. Regular activities of daily living can typically be resumed between 4–6 weeks postoperative, as well as transitioning from a flat, rigid postoperative shoe to a regular supportive closed shoe. Low-impact exercise (such as swimming, recumbent bike, or similar) is typically safe to initiate between 6–10 weeks postop depending upon the procedure performed. Ballistic or high-impact athletic activity is typically resumed between 3–4 months postoperatively, or should be restricted until serial radiographic healing of the operative site is noted.
Common Pitfalls to Avoid
Due to the steep learning curve associated with MIS foot and ankle surgery, there are common complications and pitfalls that surgeons should keep in mind. In my observation, some of the more common complications associated with MIS procedures include: nerve injury, iatrogenic wound complications, thermal injury to soft tissue or osseous structures, unstable fixation, and mal/delayed/nonunion of osteotomy or arthrodesis sites. As an additional caveat, surgeons should make sure to check deformity correction and internal fixation in multiple planes using intraoperative fluoroscopy. Speaking from experience, there are situations in which a dorsoplantar foot view can appear perfect, but on a lateral foot view the fixation is completely off. Additionally, a patient consenting for MIS foot and ankle surgery should be informed of the potential for conversion of the MIS procedure to an open procedure in situations where the surgery ultimately can not be accomplished through a MIS approach. The purpose of this is 2-fold as it gives the surgeon a safety net or “plan B” to fall back upon, but it also preemptively (and appropriately) warns a patient of this possibility during the consent process for the proposed procedure.
In Conclusion
MIS foot and ankle surgery offers patients many potential benefits over traditional open procedures, including tiny, cosmetically pleasing scars, decreased postoperative pain (possibly resulting in less narcotic use), less postoperative joint stiffness, immediate weight-bearing, and an overall quicker recovery with earlier return to regular shoe gear, work, and activity. There exists a high learning curve for these techniques, but a number of factors can aid in overcoming this challenge. These include saw bone and cadaver labs to practice MIS techniques and procedures (familiarizing surgeons with instrumentation and fixation, developing appropriate muscle memory), spending time with high-volume MIS surgeons, critically reviewing current MIS literature, utilizing tools such as external jig systems and preoperative templates to anticipate procedural steps or definitive fixation, and using fluoroscopy in multiple planes for confirmation of deformity correction and appropriate fixation. Do not be afraid to convert MIS procedures to open surgeries when first starting. The best way to overcome pitfalls associated with MIS foot and ankle surgery is to prevent them. Only then will both surgeon and patient reap the benefits of performing foot and ankle surgery through a MIS approach versus employing traditional open techniques.
Dr. Abicht is a board-certified foot and ankle surgeon practicing at Gundersen Health System (GHS) in La Crosse, WI. He is a Fellow of the American College of Foot and Ankle Surgeons and serves as department chair for the Podiatric Medicine and Surgery Department at GHS. Dr. Abicht serves on the editorial board for multiple journals. Disclosures: Dr. Abicht is a consultant for, and/or receives royalties from, the following entities: Novastep®, In2Bones (A ConMed Company), Acera Surgical, Surgical Fusion Technologies, and Avitus® Orthopedics. Dr. Abicht is also an editorial board member for FASTRAC and Podiatry Today.
References
1. Jeyaseelan L and Malagelada F. Minimally invasive hallux valgus surgery – a systematic review and assessment of state of the art. Foot Ankle Clin N Am. 2020;25(3):345-359.
2. Ketao L, Ding S, Sun C, Sun S, and Zhang M. Minimally invasive vs. open surgery for hallux valgus: a meta-analysis. Front Surg. 2022;9:1-12.
3. Kaufmann G, Mörtlbauer L, Hofer-Picout P, Dammerer D, Ban M, and Liebensteiner M. Five-year follow-up of minimally invasive distal metatarsal chevron osteotomy in comparison with the open technique – a randomized controlled trial. J Bone Joint Surg Am. 2020;102(10):873-879.
4. Palmanovich E, Ohana N, Atzmon R, Slevin O, Brin Y, Feldman V, and Segal D. MICA: a learning curve. J Foot Ankle Surg. 2020;59(4):781-783.
5. Jowett CRJF, Bedi HSF. Preliminary results and learning curve of the minimally invasive chevron akin operation for hallux valgus. J Foot Ankle Surg. 2017;56(3):445-452.
6. Mikhail C, Markowitz J, Di Lenarda L, Guzman J, and Vulcano E. Clinical and radiographic outcomes of percutaneous chevron-akin osteotomies for the correction of hallux valgus deformity. Foot Ankle Int. 2022; 43(1):32–41.
7. Abicht B. Percutaneous first metatarsophalangeal joint arthrodesis. FASTRAC. 2021;1(3): https://doi.org/10.1016/j.fastrc.2021.100041
8. Bauer T, Lortat-Jacob A, Hardy P. First metatarso-phalangeal joint percutaneous arthrodesis. Orthop Traumatol Surg Res. 2010;96(5):567-73.
9. Fanous R, Ridgers D, Sott, A. Minimally invasive arthrodesis of the first metatarsophalangeal joint for hallux rigidus. Foot Ankle Surg. 2014;20(3):170-3.
10. Hodel S, Viehofer A, Wirth S. Minimally invasive arthrodesis of the first metatarsophalangeal joint: a systematic review. Foot Ankle Surg. 2020;26(6):601-6.
11. Sott A. Minimally invasive arthrodesis of 1st metatarsophalangeal joint for hallux rigidus. Foot Ankle Clin. 2016;21(3):567-76.
12. Furmanek J, Rahnama-Vaghef A, and Siddiqui N. What role might minimally invasive surgery (MIS) play in Charcot reconstruction? Podiatry Today. 2021; 34(7):32–38.
13. Reddy S, Schipper O, and Li J. The effect of chilled vs room-temperature irrigation on thermal energy dissipation during minimally invasive calcaneal osteotomy of cadaver specimens. Foot Ankle Orthopaedics. 2022;7(4):1-5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}