

Use of Remote Monitoring to Detect CRT Under-Pacing
Introduction
Since the publication of the MADIT II trial, cardiac devices have played a prominent role in the reduction of mortality of the heart failure patient.1 With the extension of life from the reduction of sudden cardiac arrest comes the progressive development of congestive heart failure, increasing the clinical complexity of these patients.
Diagnostic data contained within these cardiac devices has proven instrumental in the management of the heart failure patient. While no study to date has shown a mortality benefit attributable specifically to heart failure diagnostics, a clear ability to risk-stratify patient populations has emerged.2 The sampling rate of the data from the PARTNERS-HF study also suggested that more frequent sampling increased the predictive capacity for heart failure hospitalization.2 The IN-TIME study was a randomized trial comparing standard care versus alert-based telemonitoring (BIOTRONIK Home Monitoring) in 716 patients with chronic heart failure with an ICD or CRT-D device.3 The primary endpoint was a composite clinical score that factored in all-cause mortality, overnight hospitalization for heart failure, a change in NYHA class, and a change in the patient global assessment (PG) score. In 12 months, the composite score worsened more in the control than the telemonitoring group (27.2% vs 18.9%; P=0.013). This difference occurred mainly because all-cause mortality was higher in the control group than the telemonitoring group (27 vs 10 deaths, respectively). The rate of all-cause mortality alone was 3.4% for Home Monitoring patients compared to 8.7% for the control group (hazard ratio [HR] 0.36, 95% confidence interval [CI], range 0.17-0.74). In a post-hoc analysis, one-year cardiovascular mortality was 2.7% for Home Monitoring patients and 6.8% for control patients (HR 0.37, CI 0.16-0.83).3
In this article, we present a case study in which close clinical supervision with the use of Home Monitoring detected CRT under-pacing in a patient, avoiding hospitalization.
Case Description
 A 65-year-old female with a longstanding history of ischemic cardiomyopathy and ventricular tachycardia (VT) presented to the clinic due to recurrent VT in January 2018. Her initial presentation of anterior myocardial infarction in 1987 at age 32 was treated with an acute percutaneous coronary intervention. She had ventricular tachycardia in 2005 necessitating implantation of an implantable cardioverter defibrillator (ICD) for secondary prevention. She was noted to have an ejection fraction of 10% after presentation with acute systolic heart failure in 2008. She underwent VT ablation in 2012 after failure of amiodarone and mexiletine — this stabilized her arrhythmia, and she received mexiletine post ablation due to hepatotoxicity with amiodarone.
A 65-year-old female with a longstanding history of ischemic cardiomyopathy and ventricular tachycardia (VT) presented to the clinic due to recurrent VT in January 2018. Her initial presentation of anterior myocardial infarction in 1987 at age 32 was treated with an acute percutaneous coronary intervention. She had ventricular tachycardia in 2005 necessitating implantation of an implantable cardioverter defibrillator (ICD) for secondary prevention. She was noted to have an ejection fraction of 10% after presentation with acute systolic heart failure in 2008. She underwent VT ablation in 2012 after failure of amiodarone and mexiletine — this stabilized her arrhythmia, and she received mexiletine post ablation due to hepatotoxicity with amiodarone.
 The patient originally received an ICD (Lumos VRT, BIOTRONIK) in 2005, and was upgraded in 2011 to a CRT-D system (Lumax 540 HF-T, BIOTRONIK) due to progressive systolic heart failure in the presence of a left bundle branch block. Her ejection fraction remained 10% following upgrade to a CRT-D. The Lumax 540 HF-T offers Home Monitoring, which collects data from the implanted device nightly with an alert system for clinically actionable items. Home Monitoring alerts allow for certain programmed conditions to trigger a warning to the clinical team, coded as yellow or red, depending on the seriousness of the issue.
The patient originally received an ICD (Lumos VRT, BIOTRONIK) in 2005, and was upgraded in 2011 to a CRT-D system (Lumax 540 HF-T, BIOTRONIK) due to progressive systolic heart failure in the presence of a left bundle branch block. Her ejection fraction remained 10% following upgrade to a CRT-D. The Lumax 540 HF-T offers Home Monitoring, which collects data from the implanted device nightly with an alert system for clinically actionable items. Home Monitoring alerts allow for certain programmed conditions to trigger a warning to the clinical team, coded as yellow or red, depending on the seriousness of the issue.
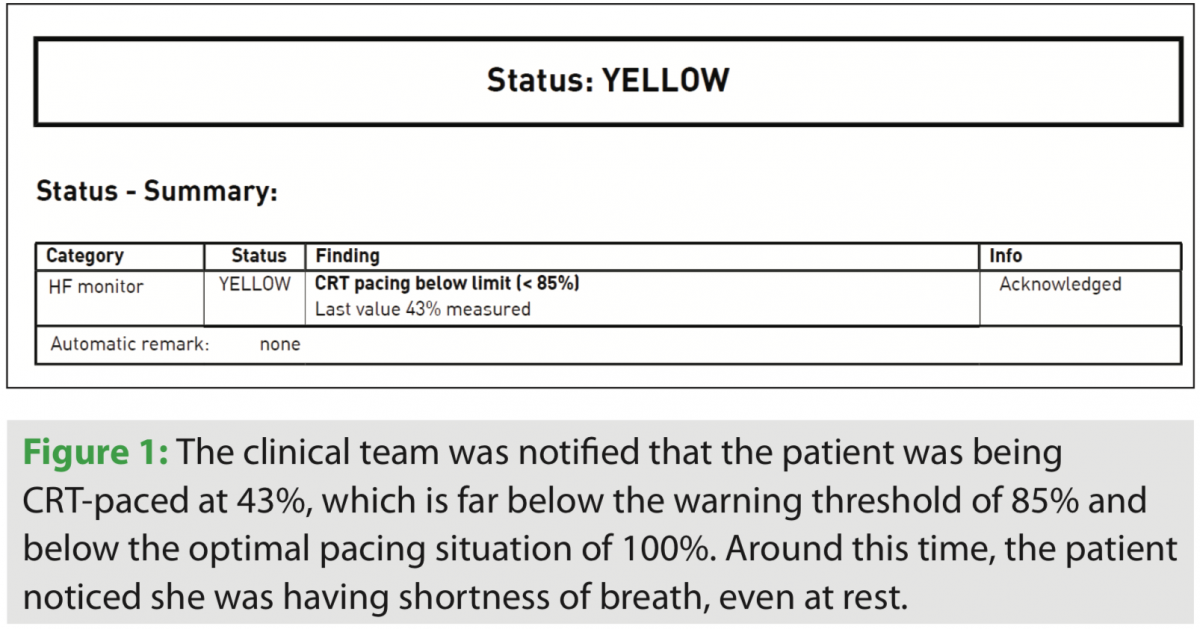
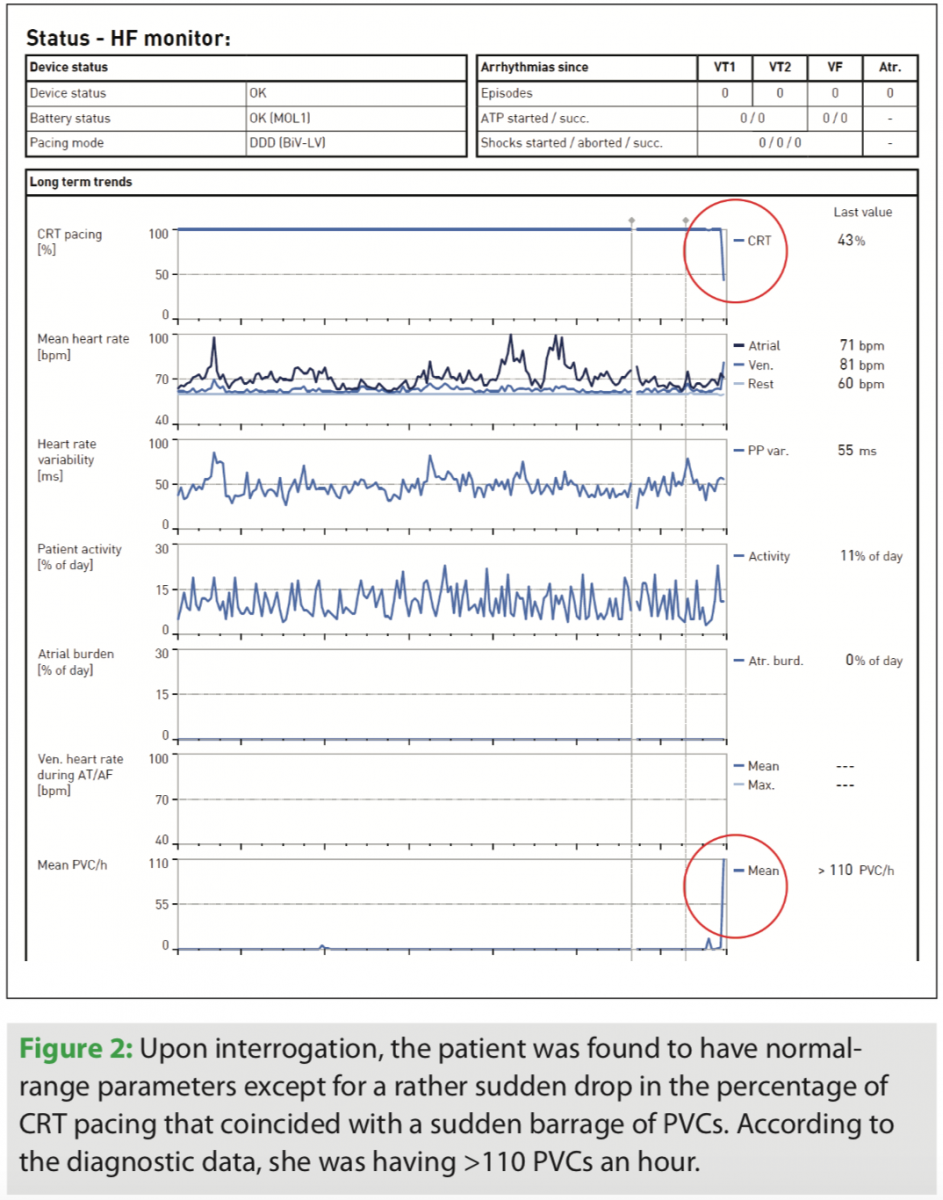
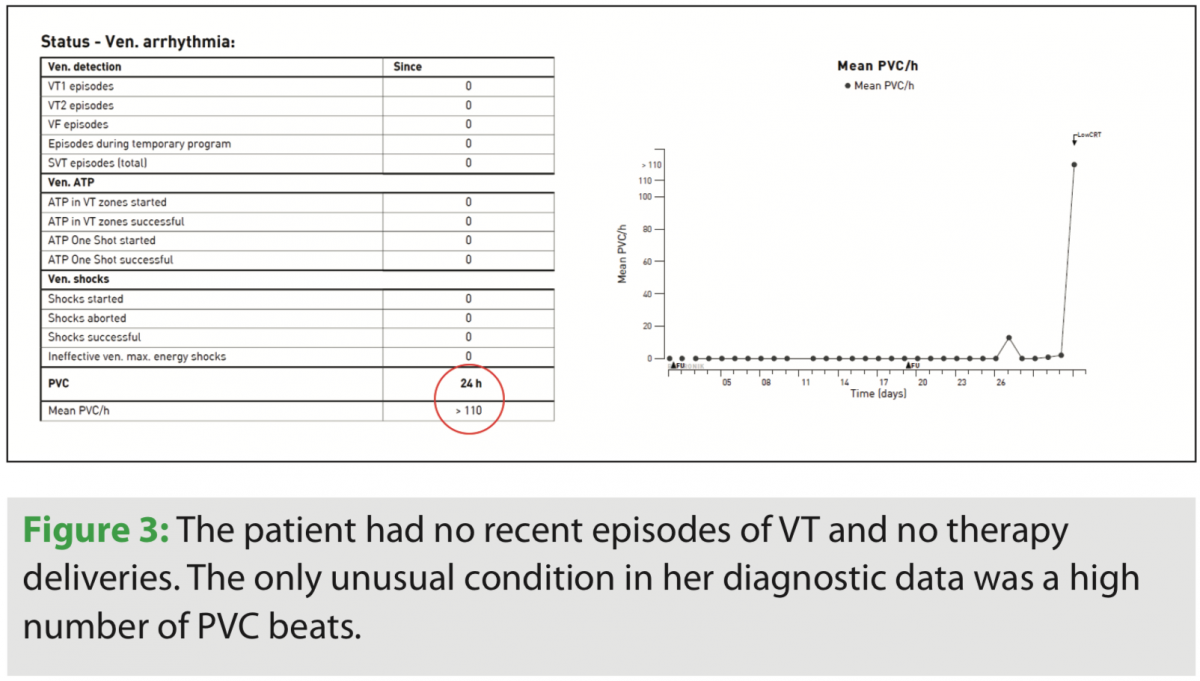 A yellow alert was received due to CRT under-pacing (<85%), whereupon the patient was called and was noted to have recently developed symptoms of dyspnea at rest (Figure 1). Prior to this yellow alert, the patient was compensated with a stable ventricular arrhythmia burden and no recent shocks (Figures 2 and 3).
A yellow alert was received due to CRT under-pacing (<85%), whereupon the patient was called and was noted to have recently developed symptoms of dyspnea at rest (Figure 1). Prior to this yellow alert, the patient was compensated with a stable ventricular arrhythmia burden and no recent shocks (Figures 2 and 3).
The patient was called to the office for a face-to-face visit. She told the clinical team that she had financial problems getting her medications and had not been taking them for approximately 1 week. Assistance was provided, the patient resumed medical therapy as prescribed, and she regained her NYHA Class II status, avoiding hospitalization.
Discussion
Heart failure patients can be complex and pose specific challenges to the clinical team. In this case, the patient had a CRT-D device, a history of myocardial infarction, left ventricular dysfunction, and a history of cardiac interventions. Managing a patient like this requires close clinical supervision and vigilance so that seemingly “minor” imbalances do not result in hospitalizations or other severe consequences. In this case, the patient struggled financially and stopped taking her medications, but did not report this to the clinic. This scenario is fairly common in clinical practice, along with other forms of nonadherence.
The IN-TIME data suggested that CRT under-pacing is a major cause of worsening heart failure in patients like this. Without the alert system, this abrupt decrease in percentage of CRT pacing would not have been noted until her next in-clinic visit or if the patient sought clinical care for her symptoms of dyspnea. The alert system allowed the clinical team to review her device data promptly and then take the necessary steps to quickly restore her medications. In the absence of remote monitoring, her clinical presentation was more likely to involve severe clinical symptoms or an emergency department visit or hospitalization. Home Monitoring with alerts provides an excellent means for clinicians to keep track of the day-to-day issues in complex heart failure patients without having them frequently come to the clinic.
Conclusion
CRT device therapy can reduce mortality in heart failure patients, and devices with Home Monitoring can help physicians manage complex heart failure patients. This brief case study demonstrates how an alert was able to detect a problem before the patient was even aware of it, and address it in such a way that avoided hospitalization for the patient. Whether or not remote monitoring can reduce heart failure mortality remains to be seen, but it plays a valuable role in the real-world clinical setting with complex heart failure patients.
Disclosures: The authors have no conflicts of interest to report regarding the content herein. Outside the submitted work, Dr. Mehta reports personal fees from BIOTRONIK as part of a speaker's bureau; Ms. Cooper reports personal fees from BIOTRONIK; Ms. Davenport reports personal fees from BIOTRONIK; and Dr. Gulati reports personal fees as a speaker and consultant for BIOTRONIK, Medtronic, and Abbott.
References
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346(12):877-883.
- Whellan DJ, Ousdigian KT, Al-Khatib SM, et al. Combined heart failure device diagnostics identify patients at higher risk of subsequent heart failure hospitalizations: results from PARTNERS HF (Program to Access and Review Trending Information and Evaluate Correlation to Symptoms in Patients With Heart Failure) study. J Am Coll Cardiol. 2010;55(17):1803-1810.
- Hindricks G, Taborsky M, Glikson M, et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet. 2014;384(9943):583-590.

