

The Journey to Achieve Zero
According to the CDC, 1.7 million Americans will acquire a healthcare-associated infection (HAI) each year; of those, 99,000 patients will die from a HAI, resulting in approximately $20 billion in annual healthcare costs.1
The long-term effects to the patient and their family carries a larger impact, as the pain and suffering of infection treatments cannot be quantified. For this reason, we diligently aim to achieve a zero percent infection rate. This may seem like an impossible task, but it is what we strive for; every day, every patient deserves the best outcome. This article shares our team’s journey towards that goal in the search for zero.
Identifying Areas of Improvement
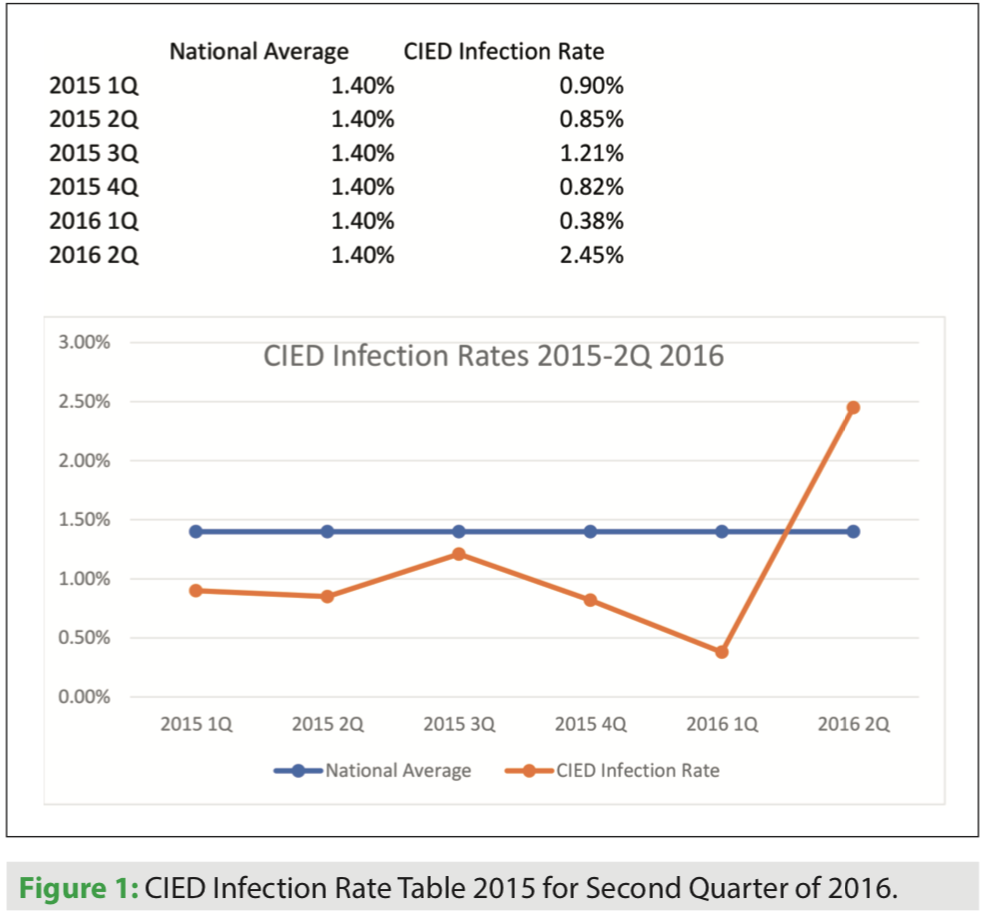 In 2015, we began to experience a rise in cardiovascular implantable electronic device (CIED) infections, which maxed out at 2.45% in the second quarter of 2016 (Figure 1). Our electrophysiology (EP) team, including lab personnel, physicians, and leadership, were concerned and began to examine every process along the continuum of a patient’s CIED implant episode of care for possible causes. We investigated infection control process adherence and changes, potential impact of new lab teammates, and physical environment concerns such as nearby construction or air handling issues. Had anything changed? At the end of the investigation, we were unable to point to any singular cause, and began to analyze each process for appropriateness and consistency. We went back to fundamentals. Therefore, the Clinical Quality, Efficiency, and Effectiveness Committee (CQE2) was created to review all facets of infection prevention processes for CIED procedures in the Sanger Heart & Vascular Institute (SHVI) Electrophysiology Laboratory.
In 2015, we began to experience a rise in cardiovascular implantable electronic device (CIED) infections, which maxed out at 2.45% in the second quarter of 2016 (Figure 1). Our electrophysiology (EP) team, including lab personnel, physicians, and leadership, were concerned and began to examine every process along the continuum of a patient’s CIED implant episode of care for possible causes. We investigated infection control process adherence and changes, potential impact of new lab teammates, and physical environment concerns such as nearby construction or air handling issues. Had anything changed? At the end of the investigation, we were unable to point to any singular cause, and began to analyze each process for appropriateness and consistency. We went back to fundamentals. Therefore, the Clinical Quality, Efficiency, and Effectiveness Committee (CQE2) was created to review all facets of infection prevention processes for CIED procedures in the Sanger Heart & Vascular Institute (SHVI) Electrophysiology Laboratory.
 The surgical hand scrub procedure was examined first. The CQE2 Committee performed a survey of current surgical hand scrub practices and analyzed responses by procedure type, surgical hand scrub product, and physical scrub time utilizing each product. The results revealed there was an excessive number of surgical scrub product options available — five in all. The survey findings determined the manufacturers’ instructions for use were not followed consistently, and it came as no surprise how products were used had been passed down from one person to the next. The preceptor was teaching a “how they were taught” method versus using the instructions for use located on the product packaging. Based on the information collected, the CQE2 Committee decided to complete a thorough review of the current scrub products. Additionally, CQE2 considered potentially introducing a new product to replace those currently available. Our team acknowledged that re-education of all staff would be necessary, and a plan to standardize future employee education would need to be developed.
The surgical hand scrub procedure was examined first. The CQE2 Committee performed a survey of current surgical hand scrub practices and analyzed responses by procedure type, surgical hand scrub product, and physical scrub time utilizing each product. The results revealed there was an excessive number of surgical scrub product options available — five in all. The survey findings determined the manufacturers’ instructions for use were not followed consistently, and it came as no surprise how products were used had been passed down from one person to the next. The preceptor was teaching a “how they were taught” method versus using the instructions for use located on the product packaging. Based on the information collected, the CQE2 Committee decided to complete a thorough review of the current scrub products. Additionally, CQE2 considered potentially introducing a new product to replace those currently available. Our team acknowledged that re-education of all staff would be necessary, and a plan to standardize future employee education would need to be developed.
 A comprehensive literature review was performed to compare the current as well as other available surgical scrub products. The literature demonstrates the superiority of alcohol-based products for antimicrobial hand scrub. A 70% alcohol waterless surgical scrub versus a chlorhexidine gluconate (CHG) 4% surgical water-aided scrub is statistically better, according to the FDA’s tentative final monograph (TFM) testing standards. Some studies have shown that alcohol with a CHG waterless surgical hand scrub provides a persistent effect at 6 hours post scrub, recommending that there be a CHG component in waterless surgical scrubs.2
A comprehensive literature review was performed to compare the current as well as other available surgical scrub products. The literature demonstrates the superiority of alcohol-based products for antimicrobial hand scrub. A 70% alcohol waterless surgical scrub versus a chlorhexidine gluconate (CHG) 4% surgical water-aided scrub is statistically better, according to the FDA’s tentative final monograph (TFM) testing standards. Some studies have shown that alcohol with a CHG waterless surgical hand scrub provides a persistent effect at 6 hours post scrub, recommending that there be a CHG component in waterless surgical scrubs.2
The use of scrub brushes was also researched. The results showed the use of surgical brushes has not been proven to provide any advantages in reducing microorganisms, but it does increase the risk of skin irritation and breakdown of the epidermis. The use of alcohol-based surgical water-aided scrubs has been shown to have immediate antimicrobial efficacy compared to CHG products, and does not require the use of scrub brushes.3
 The CQE2 Committee, in collaboration with hospital infection preventionists, decided to utilize a waterless surgical hand scrub product as the primary method for surgical scrub. Avagard™ (3M) is currently used as our waterless product. Avagard has CHG 1% and ethyl alcohol 61% as well as moisturizers that prevent skin drying with use. Our team found this product easy to use, and there is no set scrub time. It is key to follow the manufacturer’s instructions when using any product. Because some teammates experience skin irritation with Avagard, the product evaluation team also chose to make two other products available: a CHG 4% surgical scrub, and Betadine (povidone-iodine) surgical scrub (Purdue Pharma L.P.). Regardless of the product chosen for use, all staff were formally re-educated on the use of each product utilizing product vendor support.
The CQE2 Committee, in collaboration with hospital infection preventionists, decided to utilize a waterless surgical hand scrub product as the primary method for surgical scrub. Avagard™ (3M) is currently used as our waterless product. Avagard has CHG 1% and ethyl alcohol 61% as well as moisturizers that prevent skin drying with use. Our team found this product easy to use, and there is no set scrub time. It is key to follow the manufacturer’s instructions when using any product. Because some teammates experience skin irritation with Avagard, the product evaluation team also chose to make two other products available: a CHG 4% surgical scrub, and Betadine (povidone-iodine) surgical scrub (Purdue Pharma L.P.). Regardless of the product chosen for use, all staff were formally re-educated on the use of each product utilizing product vendor support.
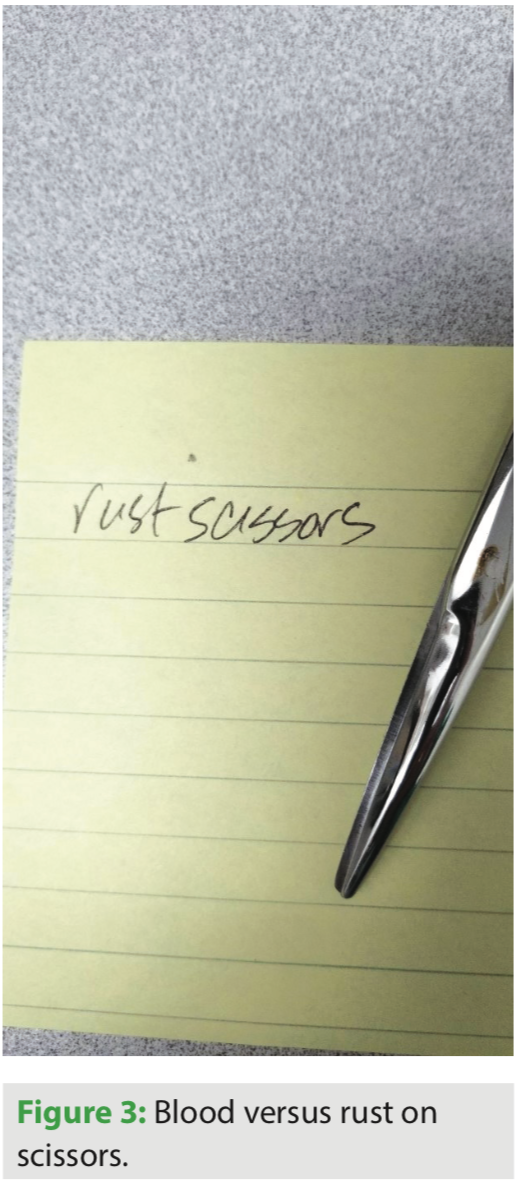
 The next area of opportunity focused on inspection of surgical instruments. Assessment of the team’s practices revealed inconsistencies with inspection processes of the surgical instrument trays and instrument rejection criteria. The team was consistent in instrument rejection for bioburden, but uncertainty was observed with respect to the presence of rust, discoloration, and pitting. It was determined that “staining” or discolored instruments are acceptable; however, rust on the instrument was cause for rejection. Pitting of the metal on instruments should also be rejected and sent for refurbishing. Standards for surgical instrument tray inspection and criteria for rejection were developed and the staff were educated. One newly introduced process included inspection of surgical instrument packaging by the circulator prior to presenting instruments to the scrub person. (Figures 2-5)
The next area of opportunity focused on inspection of surgical instruments. Assessment of the team’s practices revealed inconsistencies with inspection processes of the surgical instrument trays and instrument rejection criteria. The team was consistent in instrument rejection for bioburden, but uncertainty was observed with respect to the presence of rust, discoloration, and pitting. It was determined that “staining” or discolored instruments are acceptable; however, rust on the instrument was cause for rejection. Pitting of the metal on instruments should also be rejected and sent for refurbishing. Standards for surgical instrument tray inspection and criteria for rejection were developed and the staff were educated. One newly introduced process included inspection of surgical instrument packaging by the circulator prior to presenting instruments to the scrub person. (Figures 2-5)
During team education, we discovered that instruments were being cleaned with normal saline versus sterile water. Using normal saline to clean the instruments may cause premature aging and breakdown of protective instrument coating, which results in pitting. We implemented a process change to fully clean instruments by soaking them in sterile water after use and removing all visible bioburden prior to spraying the instruments with pre-enzyme cleaner and transport to sterile processing. Our team also learned that some teammates believed that staff from the sterile processing department were fully responsible for the cleanliness of the surgical instruments. All teammates are responsible for maintenance of surgical instruments, as it takes all teams doing their best to maintain the integrity of our instruments. We discovered that engagement of the entire team will provide the best end-product.
Focus was also placed on reducing the number of individual products that need to be dropped on the sterile field. The team worked with our vendor, Cardinal Health, to update our implant packs to include all items except sutures, sheaths, gowns, and gloves (as these items vary by clinician). Reducing the quantity of items to be opened individually reduces the risk of contamination and improves overall lab efficiency, as back table preparation is reduced. A mayo stand cover was added to the pack to facilitate opening and inspecting instruments off the back table. Each step helps staff meet expectations. This is important to remember, as processes and expectations are changed. Providing the team with the appropriate tools facilitates successful process change implementation.
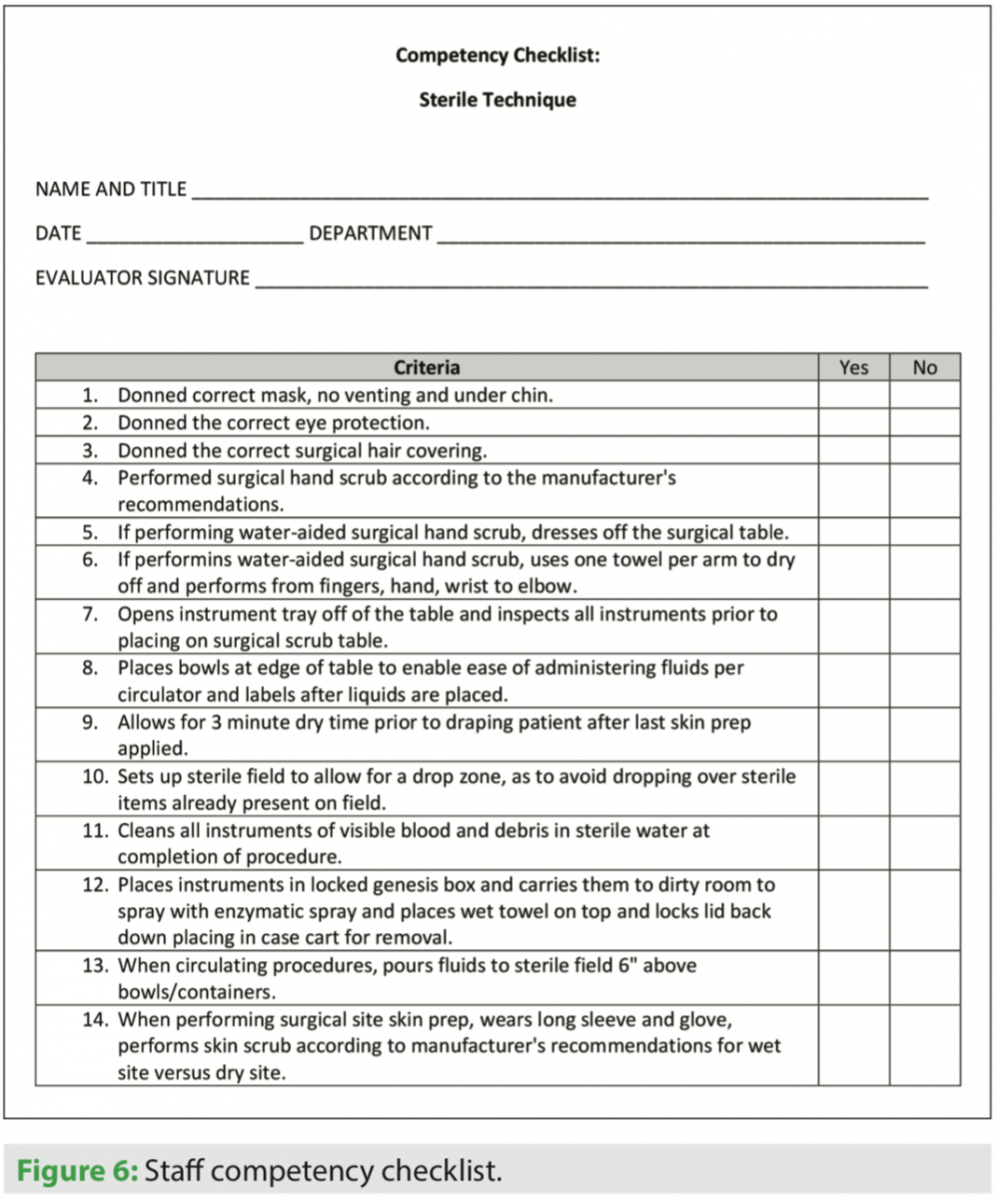 Staff education was developed using evidence-based practice guidelines from the Association of periOperative Registered Nurses (AORN) practice standards and recommendations. It became important to have one standard and one person deliver the same message to staff. A PowerPoint presentation is now updated annually to include any changes in the current AORN recommendations, which is then reviewed with staff. The staff must prove annual competency in the area of surgical site skin prep and their overall sterile technique. This checklist is shown in Figure 6.
Staff education was developed using evidence-based practice guidelines from the Association of periOperative Registered Nurses (AORN) practice standards and recommendations. It became important to have one standard and one person deliver the same message to staff. A PowerPoint presentation is now updated annually to include any changes in the current AORN recommendations, which is then reviewed with staff. The staff must prove annual competency in the area of surgical site skin prep and their overall sterile technique. This checklist is shown in Figure 6.
All new teammates are required to go through the Sterile Technique Skills Lab prior to scrubbing any case in the electrophysiology lab. This gives the new teammate a safe zone to practice surgical hand scrubbing, gowning, gloving, inspecting of instruments, preparing a back table, and draping a simulated patient. The Sterile Technique Skills Lab provides one-on-one education and opportunity for new teammates to master sterile technique and scrub practices for EP procedures. Validating competence for sterile technique reinforces the value and importance of these practices. The Sterile Technique Skills Lab is provided by the same staff member every time. Again, the value of the skills lab ensures the consistency and integrity of the procedural education. The message given to teammates is that surgical consciousness begins and ends with them. The Sterile Technique Skills Lab requires up to 2.5 hours, and no shortcuts are ever taken. All teammates have gone through this skills lab.
Prior to the patient’s arrival in the procedure room, a thorough surgical site inspection is performed by the charge person. This person removes all hair from the site and all adhesive from the patient’s skin if noted. If any skin breakdown is noted, the charge person will notify the procedure physician for further assessment prior to bringing the patient to the lab. It is important to document the assessment and any interventions taken. Patients will receive the appropriate antibiotics within the determined timeframe prior to incision. We follow Surgical Care Improvement Project (SCIP) recommendations for antibiotic administration.4
All staff in the CIED procedure are required to wear long-sleeved hospital provided scrub jackets in the procedure room along with surgical head covering, beard covering, and masks. Surgical skin prep is done with ChloraPrep™ (BD). When performing the surgical skin prep, staff are required to wear clean gloves as well as ensure that all staff’s skin is covered by the scrub jacket and gloves. The surgical skin prep is performed for 30 seconds each time for a total of two times, with the recommended dry time of three minutes prior to draping, according to manufacturer’s instructions.
Reducing the amount of staff members and vendors in the procedure room is also an element that is valuable to consider. We sometimes still struggle with this area, but we ask that only one vendor be in the room unless they are providing necessary training to their staff. The more bodies there are in the procedure room increases the amount of movement, which increases contamination risk.
The discharge process is also very important. All patients receive post-CIED care instructions from one dedicated team of nurses. In our hospital, nurses from the Cardiac Rehab Team complete this process. Our CIED discharge process provides specific and consistent instruction for post-hospital care, and follow-up appointments for incision checks and device assessment are made prior to discharge.
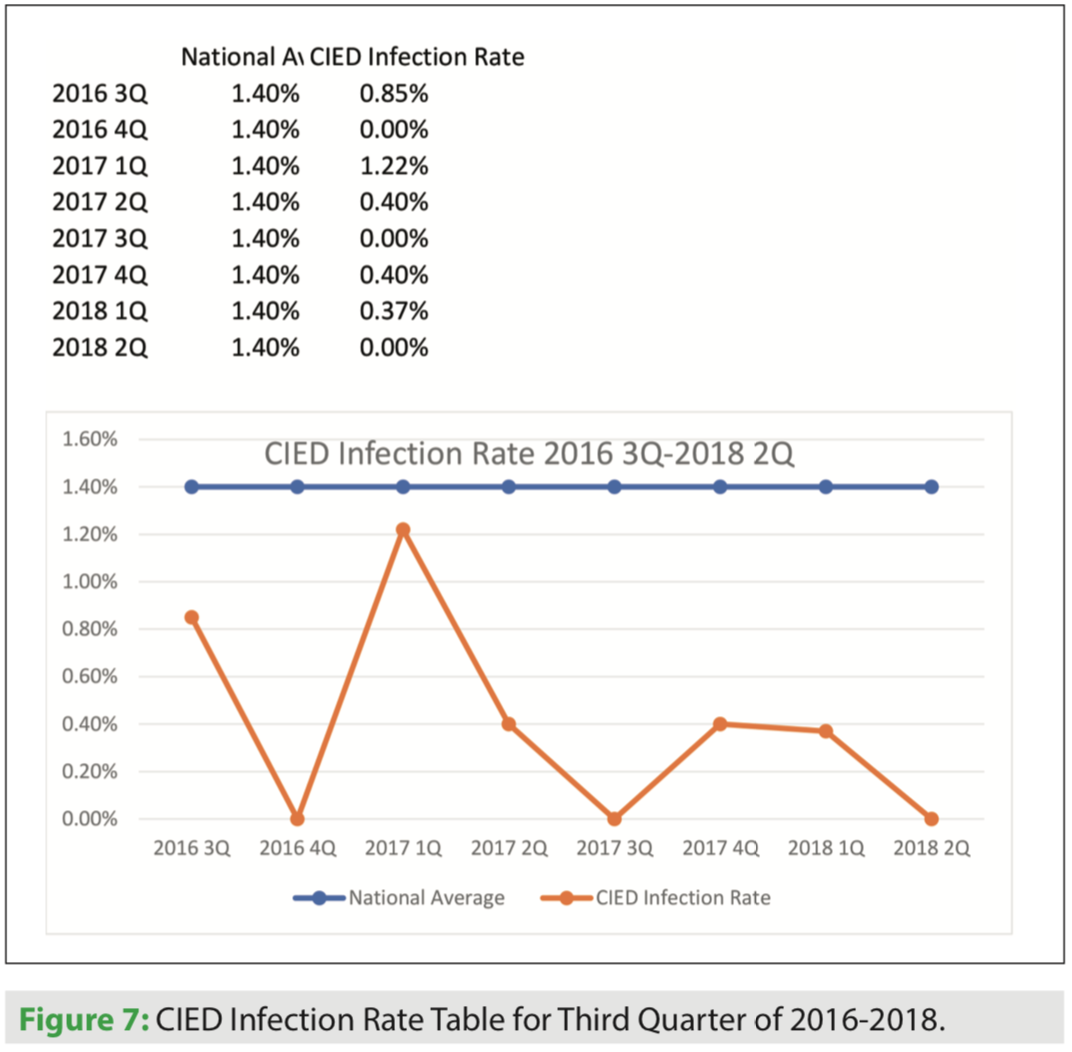 The final piece is the Device Clinic visit. It is extremely important to have experienced nurses assessing the incision site at follow-up. The incision is assessed for approximation, signs of infection, and presence of hematoma. These nurses are educated on the removal of any possible sutures that may be noted during the 7- to 10-day follow-up. This is performed by donning clean gloves, wiping the site with alcohol, and using a one-time use suture removal kit. If the nurse is unable to remove the suture for any reason or they have any concern about the healing of the incision, they can consult one of the EP nurse practitioners or physician assistants to evaluate the patient. Our SHVI Device Clinic nurses and specialist, many who are certified as cardiac device specialists, have many years of knowledge and experience in CEID management, and are a huge asset to the team. (Figure 7)
The final piece is the Device Clinic visit. It is extremely important to have experienced nurses assessing the incision site at follow-up. The incision is assessed for approximation, signs of infection, and presence of hematoma. These nurses are educated on the removal of any possible sutures that may be noted during the 7- to 10-day follow-up. This is performed by donning clean gloves, wiping the site with alcohol, and using a one-time use suture removal kit. If the nurse is unable to remove the suture for any reason or they have any concern about the healing of the incision, they can consult one of the EP nurse practitioners or physician assistants to evaluate the patient. Our SHVI Device Clinic nurses and specialist, many who are certified as cardiac device specialists, have many years of knowledge and experience in CEID management, and are a huge asset to the team. (Figure 7)
Summary
 As a result of implementing these processes, we have reduced SHVI’s CIED infection rate to 0.19% in YTD 2018, which is well below the national average of 1.4%. We pride ourselves on providing the best care we can to our patients, and this requires daily dedication from the whole team. This is our journey to achieve zero!
As a result of implementing these processes, we have reduced SHVI’s CIED infection rate to 0.19% in YTD 2018, which is well below the national average of 1.4%. We pride ourselves on providing the best care we can to our patients, and this requires daily dedication from the whole team. This is our journey to achieve zero!
Disclosure: The author has no conflicts of interest to report regarding the content herein.
References
- CDC at Work: Preventing Healthcare-Associated Infections. CDC. Available online at https://bit.ly/2q4SW9y. Accessed October 12, 2018.
- Macinga D, Edmonds S, Campbell E, McCormack R. Comparative efficacy of alcohol-based surgical scrubs: the importance of formulation. AORN J. 2014;100(6):641-650.
- Shen N, Pan S, Sheng W, et al. Comparative antimicrobial efficacy of alcohol-based hand rub and conventional surgical scrub in a medical center. J Microbiol Immunol Infect. 2015;48(3):322-328.
- Heuer A, Kossick M, Riley J, Hewer I. Update on guidelines for perioperative antibiotic selection and administration from the Surgical Care Improvement Project (SCIP) and American Society of Health-System Pharmacists. AANA Journal. 2017;85(4):293-299.

