

Hybrid Ablation for a Patient With Persistent Atrial Fibrillation and Prior Coronary Artery Bypass Grafting Surgery


Atrial fibrillation (AF) is a common arrhythmia affecting 1-2% of the general population.1,2 Rhythm control has been shown to improve quality of life, but has been elusive for patients with non-paroxysmal AF.3 Catheter ablation techniques offer suboptimal success rates for rhythm control in certain cases of persistent atrial fibrillation.4 While the Cox-Maze procedure has been described and performed for over 30 years, many consider it too invasive a procedure for rhythm control outside of concomitant heart surgery. Hybrid techniques involving a combination of minimally invasive surgical epicardial ablation paired with endocardial catheter techniques have evolved over the last several years to improve the rhythm outcomes, while reducing invasiveness in this challenging population. This case describes a patient who had highly symptomatic persistent atrial fibrillation and a prior coronary artery bypass grafting (CABG) 2 years before.
Case Presentation
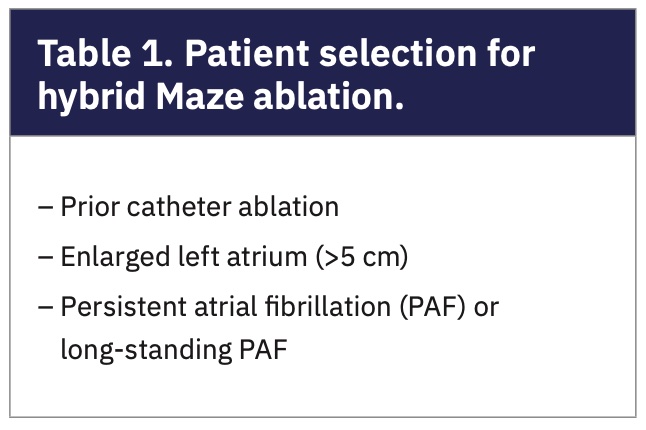
The patient is a 67-year-old male with congestive heart failure (CHF), hypertension (HTN), peripheral arterial disease (PAD), and coronary artery disease, status post CABG 2 years prior to presentation. He complained of a decline in energy and exertional dyspnea, and was found to have AF with a rate of 84 on EKG in the office, of which he did not know the duration. The patient is a retired district attorney who still practices law part time. Two-week rhythm monitor revealed 100% AF burden, and because he had a CHA2DS2-VASc of 4 (age >65, HTN, PAD, CHF), he was started on apixaban. He subsequently had 2 cardioversions with short-term success over the next few months. While ultimately unsuccessful, he did feel significant improvement while in normal sinus rhythm (NSR). His echo showed an ejection fraction of 45%, mild to moderate mitral regurgitation, and severe left atrial (LA) enlargement with a LA diameter of 5.6 cm. Since he had persistent to likely longstanding persistent atrial fibrillation refractory to cardioversion and antiarrhythmic drugs (AAD), in addition to severe LA enlargement, he was not considered to be a good candidate for catheter ablation due to the high likelihood of failure. The patient was referred for surgical consideration of a hybrid AF ablation (Table 1).
He was taken to the operating room for the first stage epicardial video-assisted thoracoscopic surgery (VATS) ablation, understanding that his case would be more complex because of his prior sternotomy and CABG procedure. Pulmonary adhesions were taken down with blunt and cautery techniques, paying special attention to avoiding phrenic nerve injury during opening of the pericardium and dissecting out the posterior heart from the adhesions. Care was also taken to avoid injuring the patent left internal mammary artery to left anterior descending bypass (LIMA-LAD) graft on the left side. The ablation involved creating radiofrequency (RF) ablation lines to perform bilateral pulmonary vein isolation (PVI), isolation of the posterior LA wall, a partial posterior mitral isthmus line, and epicardial ligation of the left atrial appendage (LAA) with an AtriClip (AtriCure, Inc.). He also had ganglionic plexi ablated and his ligament of Marshall divided as a routine part of the ablation (Figure 1). The patient was cardioverted to NSR at the completion of the procedure, and testing revealed exit block from bilateral pulmonary veins and left atrial posterior wall (Figure 2). His hospital course was uneventful. Bilateral 19 French (Fr) chest tubes were removed per routine on POD #1. He was discharged home on POD #2 in NSR on amiodarone and apixaban. On POD #53, he developed atrial flutter that was successfully treated with cardioversion.
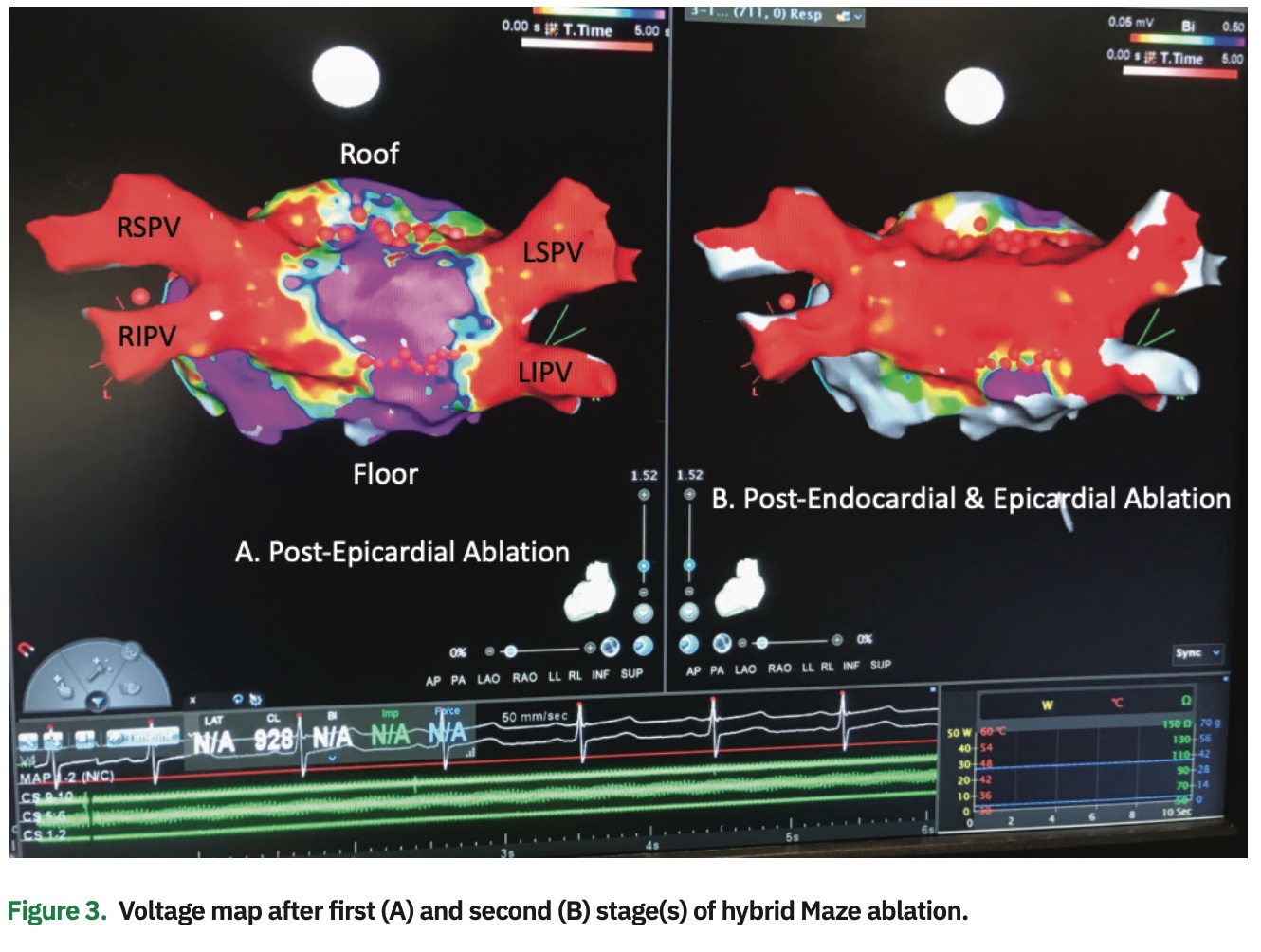
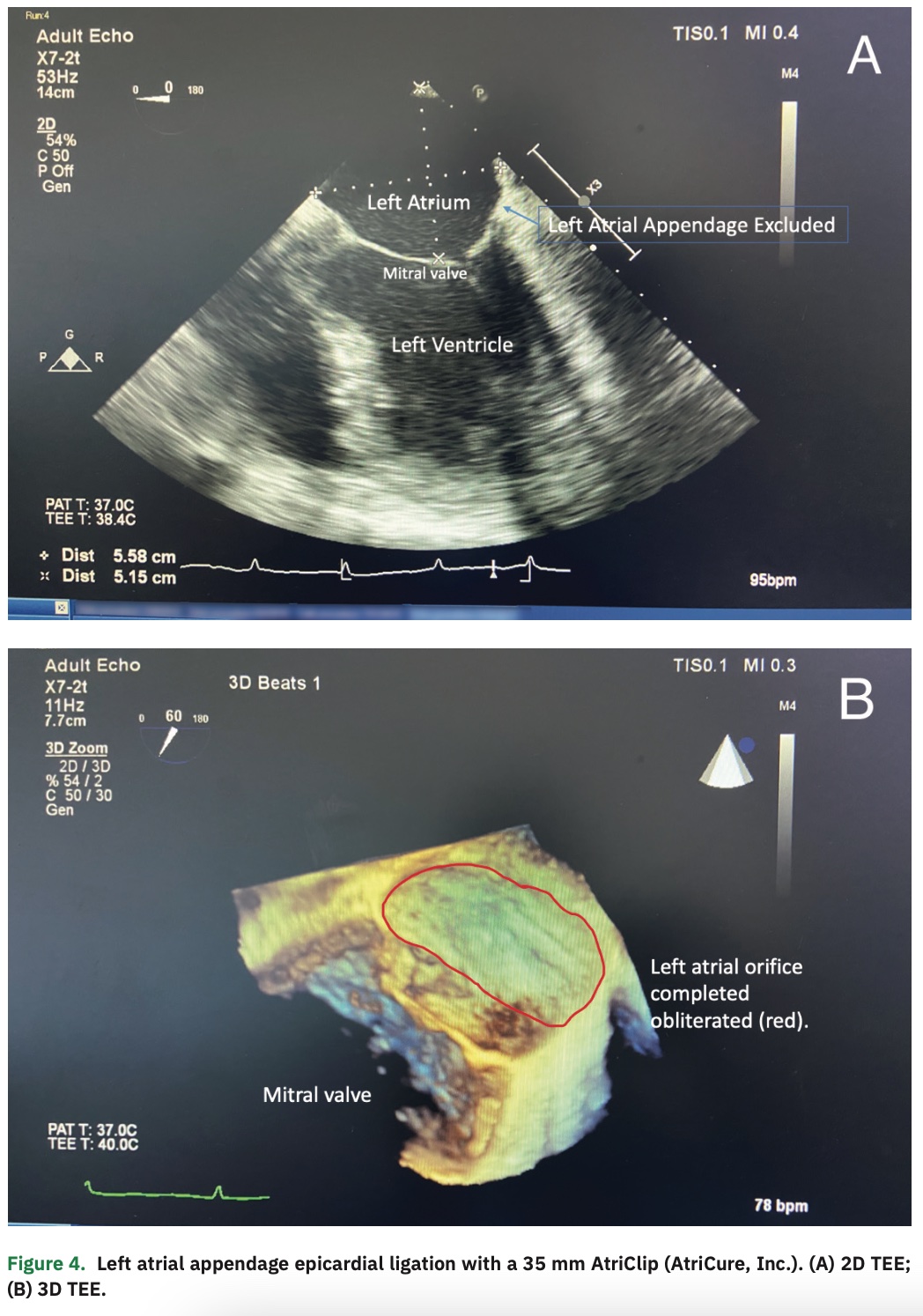
On POD #57, he returned to the EP lab with his electrophysiologist for the scheduled second stage of his hybrid ablation. His ablation was performed using standard mapping and ablation techniques. Mapping revealed well-isolated bilateral pulmonary veins with small reconnections of the roof and floor ablation lines on the right side that were successfully ablated to silence the posterior left atrial wall (Figure 3). The previously created partial mitral isthmus line was completed as well as a cavotricuspid isthmus (CTI) line, both of which confirmed bidirectional block and no recurrent atrial tachyarrhythmias with pacing and isoproterenol challenge. His LAA was found to be well occluded on transesophageal echocardiography (TEE) (Figure 4). He was discharged later that day on amiodarone and apixaban. He maintained sinus rhythm, and amiodarone and apixaban were discontinued 3 months later. The patient continues to maintain NSR 5 years later, without any symptoms of recurrence and normal annual 2-week rhythm monitors. He has significant improvement in his functional capacity, and has returned to activities such as skiing without difficulty.
Discussion
This case describes a 67-year-old male with highly symptomatic persistent atrial fibrillation that was affecting his quality of life. Having failed conventional rhythm control strategies, he elected to have a hybrid ablation, which successfully restored long-term sinus rhythm and allowed him to stop antiarrhythmic meds and anticoagulation (OAC). While this approach is more invasive than catheter ablation alone, it proves very efficacious and durable.
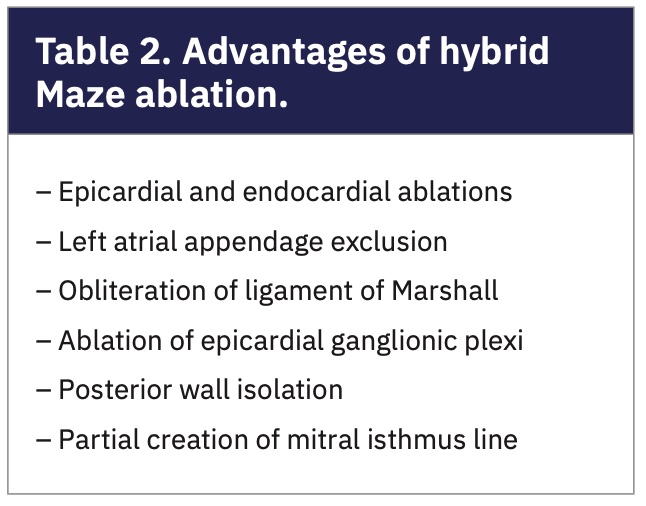
Using a hybrid team approach (Figure 3), we have performed nearly 500 hybrid Maze ablations since 2013 at our arrhythmia center. We have had excellent results, with nearly 80% restoration of NSR off AAD with up to 3-year follow-up.5 This approach has been associated with minimal complications, with less than a 5% major complication rate. Most patients are often discharged home on POD #2, and many are able to discontinue their AAD and OAC within 3 months. As our program has evolved, we have expanded to higher risk patients, including patients who have had prior open-heart surgery. In our experience, these patients have not revealed any additional risk; however, it is important to recognize that increased experience and technical skill are required for these cases. In fact, we have performed more “redo” VATS ablations than most centers have done non-redo ablations. In this report, we highlight what can be accomplished at a high-volume center experienced in hybrid and surgical approaches to AF ablation. The many advantages of hybrid ablation should be considered with all complex AF patients (Table 2).
Our center has performed hybrid ablations on patients from over 12 different states. This likely highlights the lack of centers available in the country for specialized multidisciplinary AF management. In most cases, the limiting factor is the surgical expertise required to perform the first stage of the hybrid ablation. For this reason, we work with many out-of-state electrophysiologists who may not have a surgeon trained in arrhythmia surgery. This way, the patient does not need to travel for the second stage of the hybrid procedure as long as they are in the care of an experienced electrophysiologist who performs AF ablation and is willing to collaborate in a hybrid approach. While this approach does require 2 procedures (epicardial surgical and endocardial catheter ablation), it has proven to be effective and safe in non-paroxysmal AF patients.6-8
This report describes a hybrid ablation using bilateral VATS surgical approach; however, the surgical part can also be performed via a subxiphoid approach as in the convergent9 procedure. We have performed this procedure with success, though in fewer numbers to be able to compare the long-term results at this time. The benefit of the convergent procedure may be in its greater adoptability by surgeons. The procedure may be enhanced by adding a LAA closure for stroke prevention and allowance of cessation of anticoagulation. The recently presented CONVERGE trial results showed superiority over catheter ablation, and the DEEP10 trial is still accruing patients at the time of this publication.
Conclusion
Hybrid AF ablation can provide excellent rhythm control results even in very challenging cases of persistent atrial fibrillation. The surgical approach can be safely performed at centers with highly experienced arrhythmia surgeons, which are currently increasing in number as more centers embrace this collaboration. Patients who have had prior cardiac surgery may be eligible for hybrid ablation approaches at specialized centers.
Acknowledgement. Thank you to Marcia Williams for the illustrations.
Disclosures: Dr. Dunnington and Dr. Kiankhooy report they are proctors, consultants, and speakers for AtriCure. Dr. Eisenberg and Carolyn Pierce, RN have no disclosures to report.
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA. 2001;285(18):2370-2375. doi: 10.1001/jama.285.18.2370
- Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013;112(8):1142-1147. doi: 10.1016/j.amjcard.2013.05.063
- Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: executive summary. J Arrhythm. 2017;33(5):369-409. doi: 10.1016/j.joa.2017.08.001
- Burkhardt JD, Di Biase L, Natale A. Long-standing persistent atrial fibrillation: the metastatic cancer of electrophysiology. J Am Coll Cardiol. 2012;60(19):1930-1932. doi: 10.1016/j.jacc.2012.05.058
- Liem LB, Dunnington GH, Pierce CL, Chang-Sing P, Kaiser DW. Keys for building a successful hybrid program for the treatment of persistent and long-standing persistent AF. EP Lab Digest. 2018;18(3):1,6-9.
- Maesen B, Pison L, Vroomen M, et al. Three-year follow-up of hybrid ablation for atrial fibrillation. Eur J Cardiothorac Surg. 2018;53(suppl_1):i26-i32. doi: 10.1093/ejcts/ezy117
- Haywood GA, Varini R, Osmancik P, et al. European multicentre experience of staged hybrid atrial fibrillation ablation for the treatment of persistent and longstanding persistent atrial fibrillation. Int J Cardiol Heart Vasc. 2020;26:100459. doi: 10.1016/j.ijcha.2019.100459
- de Asmundis C, Chierchia G-B, Mugnai G, et al. Midterm clinical outcomes of concomitant thoracoscopic epicardial and transcatheter endocardial ablation for persistent and long-standing persistent atrial fibrillation: a single-centre experience. Europace. 2017;19(1):58-65. doi: 10.1093/europace/euw026
- DeLurgio DB, Crossen KJ, Gill J, et al. Hybrid convergent procedure for the treatment of persistent and long-standing persistent atrial fibrillation: results of CONVERGE clinical trial. Circ Arrhythm Electrophysiol. 2020;13(12):e009288. doi: 10.1161/CIRCEP.120.009288
- Dual epicardial endocardial persistent atrial fibrillation (AF) study (Staged DEEP). ClinicalTrials.gov. Published May 17, 2017. Accessed March 31, 2021. https://clinicaltrials.gov/ct2/show/NCT01661205

