

Ventricular Pacing Redundancy Revisited: Brief Case
Introduction
Cardiac resynchronization therapy (CRT) typically employs a right and a left ventricular lead in order to pace the heart and improve heart failure. We report a case of a biventricular device being utilized in another manner, in which two right ventricular leads were used to provide ventricular pacing redundancy (VPR) in a patient who was entirely pacemaker dependent. This case illustrates and reviews the importance of having a second redundant ventricular lead in the event of lead failure.
Case Report
A 41-year-old female nurse presented to Winthrop-University Hospital with a history of syncope, drug refractory supraventricular tachycardia, previous AV node ablation with resultant complete heart block, and a permanent pacemaker. The patient had two FineLine™ leads (Model 4469, Guidant Corp.) implanted in 2004. She now presents with a fractured right atrial lead for lead revision and device replacement. The patient was very nervous about the procedure and had a premonition that there was a potential problem in her normally functioning ventricular lead. Interrogation of the device showed normal right ventricular pacing thresholds and impedance prior to the surgery. She was told that the lead would not be revised unless a problem was identified. In addition, she was completely pacemaker dependent and had no underlying escape rhythm.
The old leads were evaluated and a visible insulation defect was identified in the right ventricular lead (Figure 1). The old right ventricular lead was repaired with a protective sleeve and attached to the left ventricular port of a biventricular pacemaker (Consulta® CRT-P, Medtronic, Inc.). New right atrial and right ventricular leads were implanted and connected to the device (the latter was connected to the right ventricular port). The new pacemaker was then placed into the pocket, which was irrigated with antibiotic solution and closed with deep and superficial suture. There were no complications. At her most recent follow-up several months later, the patient had no complaints and the wound was well healed.  Both right ventricular leads were performing within their specifications with acceptable thresholds.
Both right ventricular leads were performing within their specifications with acceptable thresholds.
Discussion
This patient had complete heart block and was entirely pacemaker dependent with no underlying escape rhythm. As a healthcare worker, she knew that if the right atrial lead could fail, the right ventricular lead could also fail. It was her preference to replace both leads from the start, but we had no other evidence of right ventricular lead failure, and without that documentation, it was hard to rationalize the added cost of placing a new right ventricular lead. However, the patient’s apprehension regarding failure of the old right ventricular lead proved correct. During the procedure, it was immediately evident that the old right ventricular lead had a visible insulation defect. Although the defect was amenable to repair, the long-term stability following repair remained uncertain. In addition, the newly implanted right ventricular lead could dislodge or develop elevated thresholds, and thereby loss of capture, with a possible catastrophic result. Therefore, we utilized the old right ventricular lead with the newly implanted right ventricular lead, and attached both to a biventricular pacing device (Figure 2). This method provides a backup if the older lead fails.
Previously, the author (TC) reported on a series of seven patients who underwent VPR, typically using a biventricular pacing device.1 It is important to note that this type of pacing is especially integral to patients who are completely pacemaker dependent — at least two of the originally described cases eventually demonstrated failure of one of the ventricular leads, and thus utilized the backup pacing feature. In the event of a failed lead without a VPR system, there exists the potential for a severely devastating outcome. By providing a fail-safe option through redundancy, those potential catastrophic events could be avoided. One of the potential limitations of a VPR configuration is the issue of device energy consumption (i.e., battery drainage when pacing via two ventricular leads). As estimated by Medtronic, pacing using a redundant configuration will result in a 20 percent decrease in battery longevity, as compared to standard pacing.1 The effects on battery life may be mitigated by using VPR only during the initial three-month post-implantation window, in which a newly implanted lead may be at risk for a rise in pacing threshold and/or lead dislodgement. Additionally, some 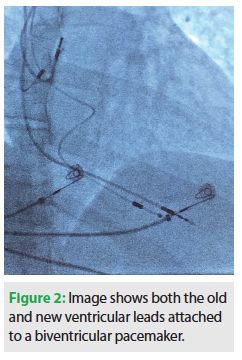 older methods of pacemaker redundancy involve simply implanting two independent pacemaker systems.2-4 With the added leads, devices and sites, these methods may increase the risk of infection.1 When utilizing a VPR system, this potential infection risk is less of an issue.
older methods of pacemaker redundancy involve simply implanting two independent pacemaker systems.2-4 With the added leads, devices and sites, these methods may increase the risk of infection.1 When utilizing a VPR system, this potential infection risk is less of an issue.
In summary, this case highlights a method of pacing referred to as ventricular pacing redundancy, which utilizes old and new ventricular leads in order to provide additional safety should one ventricular lead fail. It is interesting to note that the patient’s initial premonition regarding failure of her essential ventricular lead proved correct during the actual procedure. It is the patient’s opinion, as a practicing nurse, that all pacemaker-dependent patients should consider VPR as their primary modality. The authors believe that this may be excessive; however, in circumstances during which an unpredictable, older, or unstable lead and a newly inserted lead are used, adaptation to a biventricular pacemaker may be prudent.
Disclosures: The authors have no conflicts of interest to report regarding the content herein.
References
- Cohen TJ, Inamdar V, Asheld W, Doorty G. Ventricular redundancy pacing to prevent loss of capture: a fail-safe for pacemaker-dependent patients. J Invasive Cardiol. 2010;22(5):247-50.
- Dodinote B. Simultaneous implantation of two pacemakers. Stimucoeur Medical. 1977;5:158.
- Iwa T, Teranaka M, Misaki T, Bando T. Double pacemaker implantation. J Thorac Cardiovasc Surg. 1980;79(2):294-300.
- Morse DP, Tarjan P, McNicholas KW, DelRossi AJ, Lemole GM. Redundant pacing: case report and review. Pacing Clin Electrophysiol. 1984;7:296-300.

