

Utilizing a Fluoroless Approach: Interview with Dr. Mansour Razminia
 In this feature interview, EP Lab Digest speaks with Dr. Razminia about his experience utilizing the Advisor™ HD Grid and EnSite Precision™ (Abbott) at Presence Saint Joseph Hospital in Elgin, Illinois.
In this feature interview, EP Lab Digest speaks with Dr. Razminia about his experience utilizing the Advisor™ HD Grid and EnSite Precision™ (Abbott) at Presence Saint Joseph Hospital in Elgin, Illinois.
Many physicians are becoming more aware of their radiation hygiene and adjusting their workflow accordingly. When did you first begin this journey, and what prompted you to do so?
I began my journey in July 2010, when I observed a fluoroless catheter ablation of AVNRT performed by two of my pediatric electrophysiology colleagues at the University of Iowa. I began pursuing fluoroless catheter ablation immediately after this visit, beginning with a case of atrial flutter the day after I came back from Iowa. I became very interested in utilizing a fluoroless technique out of a concern to reduce radiation exposure to my patients, staff, and myself.
How many and what kinds of ablation cases have you performed using only a mapping system and intracardiac echocardiography (ICE)?
 Since December 2010, I have performed over 2000 consecutive procedures without using any fluoroscopy. I have ablated all arrhythmia types presenting to my lab utilizing the fluoroless technique except those requiring epicardial access.
Since December 2010, I have performed over 2000 consecutive procedures without using any fluoroscopy. I have ablated all arrhythmia types presenting to my lab utilizing the fluoroless technique except those requiring epicardial access.
Do you have a preference for a particular mapping / ICE combination system for your fluoroless workflow? If so, why?
While I have performed fluoroless catheter ablation with the EnSite Precision (Abbott) and CARTO (Biosense Webster, Inc., a Johnson & Johnson company) cardiac mapping systems, my personal preference is the EnSite system. I also use the ViewFlex ICE catheter, which I find offers astoundingly good quality images.
How do you feel ICE has helped your ablation cases in ways beyond simply reducing fluoro exposure? Are there views beyond the standard views that you use frequently?
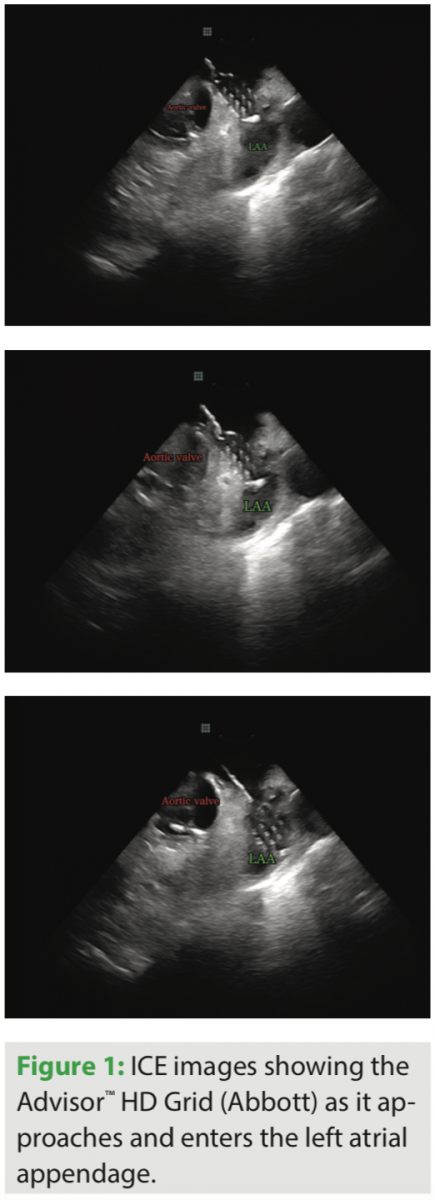
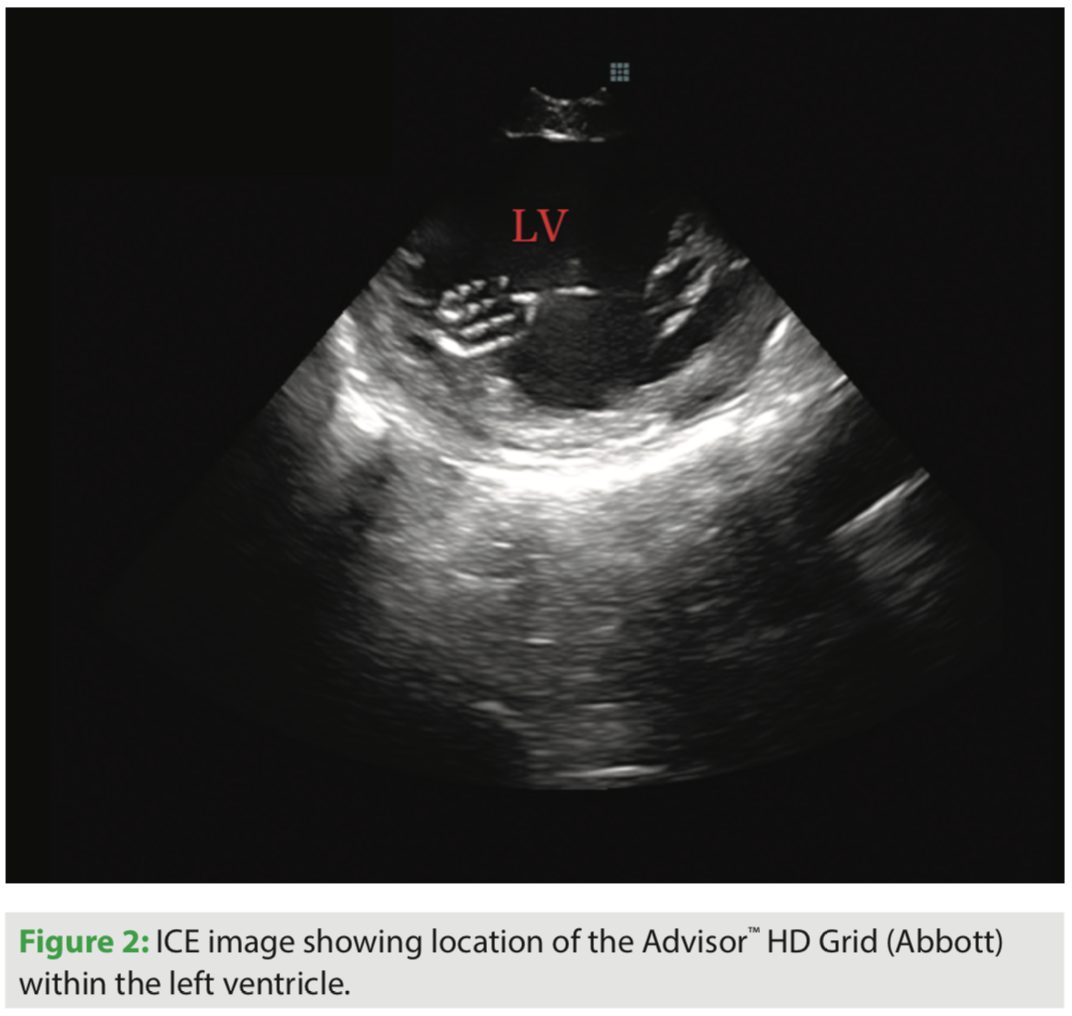 Beyond simply reducing fluoro exposure, I feel the use of ICE has significantly reduced my procedure time and complication rate, as well as improved my success rate. I use a number of non-standard views to optimize my ablation procedures. I routinely place the ICE catheter inside the left atrium for all left atrial procedures. If needed, for better visualization when addressing left ventricular tachyarrhythmias, I place the ICE catheter within the left ventricle. I frequently position the ICE catheter within the right ventricular outflow tract to address right ventricular outflow tract arrhythmias, and place the ICE catheter within the coronary sinus to improve visualization of the left atrium, left atrial appendage, and left ventricle.
Beyond simply reducing fluoro exposure, I feel the use of ICE has significantly reduced my procedure time and complication rate, as well as improved my success rate. I use a number of non-standard views to optimize my ablation procedures. I routinely place the ICE catheter inside the left atrium for all left atrial procedures. If needed, for better visualization when addressing left ventricular tachyarrhythmias, I place the ICE catheter within the left ventricle. I frequently position the ICE catheter within the right ventricular outflow tract to address right ventricular outflow tract arrhythmias, and place the ICE catheter within the coronary sinus to improve visualization of the left atrium, left atrial appendage, and left ventricle.
Over the time you have been using a fluoroless approach, there have been many introductions of new technologies such as contact force catheters and high-density mapping catheters. When adopting new technologies in the lab, how do you build them into your existing workflow?
 I have not yet incorporated contact force-sensing catheters into my routine workflow, but plan on doing so once a bidirectional contact force-sensing ablation catheter becomes available on the EnSite platform. Because of my familiarity with intracardiac ultrasound, I have found incorporating new technologies to be relatively smooth and straightforward.
I have not yet incorporated contact force-sensing catheters into my routine workflow, but plan on doing so once a bidirectional contact force-sensing ablation catheter becomes available on the EnSite platform. Because of my familiarity with intracardiac ultrasound, I have found incorporating new technologies to be relatively smooth and straightforward.
Have you incorporated new technology such as the Advisor HD Grid catheter into your workflow? If so, could you give an example with a recent case?
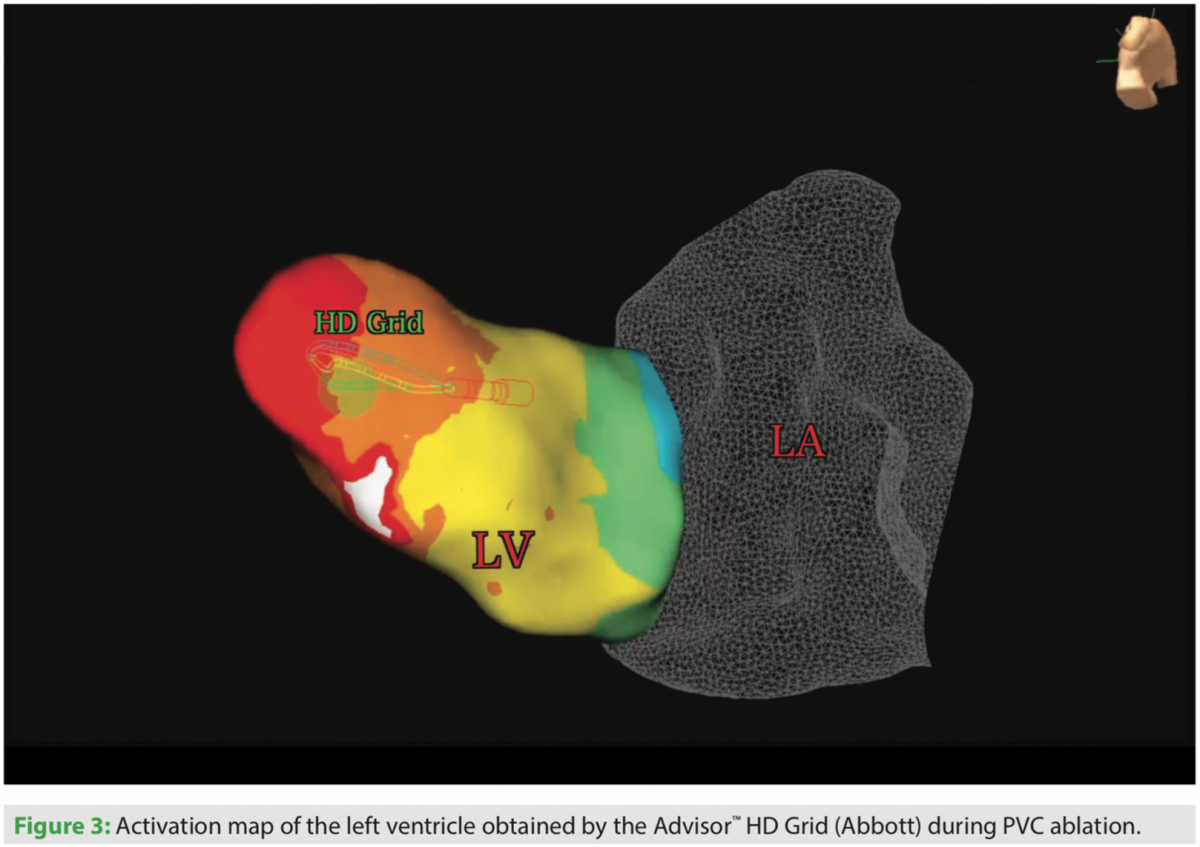
 I have been using the Advisor HD Grid for the past 6 months, and have been pleased with how this catheter has helped create detailed maps in a relatively short amount of time. I have found this catheter to be particularly useful for ablation of ventricular tachycardia and atrial tachycardia. I recently performed ablation of a PVC originating from the posteromedial papillary muscle and found that use of this catheter resulted in rapid acquisition of a very accurate activation map.
I have been using the Advisor HD Grid for the past 6 months, and have been pleased with how this catheter has helped create detailed maps in a relatively short amount of time. I have found this catheter to be particularly useful for ablation of ventricular tachycardia and atrial tachycardia. I recently performed ablation of a PVC originating from the posteromedial papillary muscle and found that use of this catheter resulted in rapid acquisition of a very accurate activation map.
How do you feel these technologies work together to provide you with the information needed to help your patients?
Incorporating intracardiac ultrasound has improved my understanding of real-time cardiac anatomy, resulting in better outcomes and shorter procedure durations in my practice. My comfort with intracardiac ultrasound has allowed me to successfully ablate arrhythmias in patients with mechanical valves as well as intracardiac devices, including biventricular devices. I have been pleased to offer my patients these complex procedures when indicated with the confidence that they would not be exposed to radiation.
What advice would you have for your peers who are considering moving to a fluoro-free approach?
I would advise them that moving to a fluoro-free approach is possible for anyone interested in taking the time to learn this technique. I would recommend taking a stepwise and gradual approach to performing fluoroless procedures. In my personal experience, I have found ICE to be invaluable in successfully and safely performing fluoroless procedures, and would encourage those interested to invest time in becoming comfortable with a variety of views. Starting with generally simpler procedures, such as ablation of CTI-dependent flutter and then gradually moving towards more complex procedures, is advised. As they rely more on ICE, they will find themselves relying less on fluoroscopy.
Is there anything else you’d like to add?
As more and more physicians are incorporating the fluoroless technique into their practice, I would be pleased to see this technique being a standard approach that is taught at the level of the fellow in training.
Disclosure: Dr. Razminia reports that he is a consultant for Abbott. Neither Dr. Razminia nor Presence Saint Joseph Hospital were compensated by Abbott for this interview.
This article is published with support from Abbott.

