

Three Coding Updates for 2013
The American Medical Association has eased the documentation burden for the most common components of ablative procedures. However, documentation requirements for complex ablative procedures have become more precise, and most add-on services have effectively been bundled into the new ablation procedures by Medicare.
Documentation Standard Eased
As originally drafted, the new ablation code definitions presented a laundry list of procedural components that would need to be documented. The atrial fibrillation ablation procedure, for example, required each of the following to be documented:
- right atrial pacing,
- right atrial recording,
- His bundle recording,
- right ventricular pacing,
- right ventricular recording,
- attempts to induce an arrhythmia, and
- multiple transseptal catheterizations.
Without each of these procedural components documented in the report, traditional coding logic forced us to add the reduced service modifier (52) to the code for the ablation (93656).
I was able to obtain clarification from the AMA that this is not the case. I asked the AMA, “Is it necessary to attach the reduced service modifier (52) to code 93656 when any of the following procedural components are not performed and documented?
- transseptal catheterizations
- induction or attempted induction of an arrhythmia
- right ventricular pacing
- right ventricular recording
- His bundle recording
The way the code is worded suggests that each of these procedures must be performed in order to report the code without the reduced service modifier. However, it is not always necessary to perform each of the above-listed components.”
The American Medical Association’s response: “modifier 52 is not necessary to be appended to the new ablation codes.”
This is good news because appending the reduced service modifier to an ablation procedure causes a loss of revenue and an extended amount of time in accounts receivable. Typically, claims submitted with this modifier are denied with a remark code indicating that additional documentation is needed to adjudicate the claim. After we submit the operative report and a cover letter explaining why the 52 modifier was applied, the payer prices the claim based on how much the procedure was reduced. Reductions in pay between 25% and 50% are not unusual. The clarification from the AMA makes it so we don’t need to affix the 52 modifier. This means we don’t need to submit a copy of the operative report, we won’t risk payment reduction, and payment will not be delayed.
An AMA representative indicated that a future publication of their CPT Assistant will contain more specifics. Perhaps the listed components of each code definition should be performed “when indicated.” Perhaps the operative report will need to illustrate that at least half of the procedural components were performed. Until further clarification is available, it is best to focus on the other topics at hand.
Add-on Services Bundled by medicare
The new ablation CPT codes (93653, 93654, and 93656) include a comprehensive, diagnostic electrophysiology study (93620) and the ablation (SVT, VT, or AF, respectively). In addition to including the EP study and ablation, the codes for AF and VT ablation include a few additional procedures:
- The AF ablation code (93656) also includes left atrial pacing and recording (93621) “when possible.”
- The VT ablation code (93654) also includes two-dimensional mapping (93609), three-dimensional mapping (93613), and left ventricular pacing and recording (93622) “when performed.”
Other than these few exceptions, coding guidelines in the CPT book indicate that it is appropriate to report add-on services in addition to the new ablation codes. One CPT book instruction says “mapping is a distinct procedure performed in addition to a diagnostic electrophysiologic study or ablation procedure and may be separately reported using 93609 or 93613.” Another instruction says “Codes 93622 and 93623 may be reported separately with 93656 for treatment of atrial fibrillation.”
As illustrated below, these add-on services add considerable revenue when compensated:
- left atrial pacing and recording (93621 – $115.00),
- left ventricular pacing and recording (93622 - $169.77),
- induction attempts following drug infusion (93623 - $156.51),
- 2D mapping (93609 - $273.20), and
- 3D mapping (93613 - $383.78).
For non-Medicare patients, you should report these add-on services when performed. The only exceptions are those mentioned above for AF and VT ablations. But for SVT ablations, they are each fair game as long as we do not report 2D and 3D mapping for the same case.
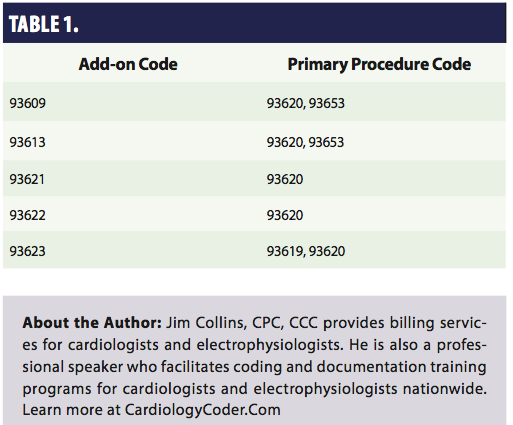 Unfortunately, CMS Transmittal 2636 prevents separate Medicare payment for these add-on codes in most cases. The transmittal requires the following, “Claims processing contractors must adopt edits to assure that Type I add-on codes are never paid unless a listed primary procedure code is also paid.” The transmittal lists the following primary procedure codes for each of our EP add-on codes (Table 1).
Unfortunately, CMS Transmittal 2636 prevents separate Medicare payment for these add-on codes in most cases. The transmittal requires the following, “Claims processing contractors must adopt edits to assure that Type I add-on codes are never paid unless a listed primary procedure code is also paid.” The transmittal lists the following primary procedure codes for each of our EP add-on codes (Table 1).
So when reporting the new ablation CPT codes (93653, 93654, and 93656) to Medicare, it will not be appropriate to report almost any of the add-on codes. The noteworthy exceptions are quite limited:
- CMS policy still permits payment for two-dimensional or three-dimensional mapping when performed during SVT ablations. Therefore, make sure to report 93609 or 93613 when mapping is performed in addition to SVT ablations (93653).
- Intracardiac echo (ICE) is another add-on code, but this round of bundling does not impact it. Make sure to report ICE (93662) when performed during any ablation.
More Precise Documentation Required
Medicare also implemented a new “Medically Unlikely Edit” for SVT ablation procedures performed subsequent to the initial ablation. CPT code 93655 is used to report ablations of each “discrete mechanism of arrhythmia which is distinct from the primary ablated mechanism, including repeat diagnostic maneuvers, to treat a spontaneous or induced arrhythmia.”
The Medically Unlikely Edit establishes that it would be unusual for this procedure code to be reported more than one time for any given operation. However, the Medically Likely Edit does not mean that code 93655 can only be reported or reimbursed one time. We just need to allocate one line on the claim form for each distinct arrhythmia that was targeted. We also need to attach a modifier to each subsequent listing of the code according to one Medicare Administrative Contractor (First Coast Service Options).
According to First Coast,1 “Since each line of a claim is adjudicated separately against the MUE value for the code on that line, the appropriate use of modifiers to report the same code on separate lines of a claim will enable a provider/supplier to report medically reasonable and necessary units of service in excess of an MUE value. The modifiers noted below will accomplish this purpose. Note: Modifier 59 should be utilized only if no other modifier describes the service.
- 76 – Repeat procedure by same physician
- 77 – Repeat procedure by another physician
- Anatomic modifiers (e.g., RT, LT, F1, F2)
- 91 – Repeat clinical diagnostic laboratory test
- 59 – Distinct procedural service”
The notation indicating that the 59 modifier should only be used if no other modifier describes the service seems to suggest that the 76 modifier would be more appropriate. However, facility-coding specialists report that payer policy frequently limits 76 modifier use to situations in which procedures are performed during different operative sessions. Because of this, it is best to stick with the 59 modifier.
Since these claims will be more prone to audit than most, make sure that your operative report clearly supports that a distinct and additional mechanism of supraventricular tachycardia is present after the preceding ablation was completed. A report that describes an isthmus line ablation following pulmonary vein isolation without mentioning that the patient has atrial flutter will probably not suffice.
Reference
- First Coast Service Options, Inc. Reporting medically reasonable and necessary units. January 11, 2013. Available online at https://medicare.fcso.com/faqs/answers/175060.asp. Accessed March 19, 2013.

