

Letter from the Editor
Sucking the Air Out of the EP Lab
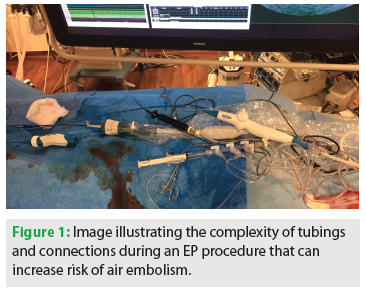 A well-known complication of cardiac procedures and cardiac surgery is air embolism. Air in the systemic circulation can embolize into the cerebral and coronary arteries. In the OR, de-airing techniques are critical to safe cardiopulmonary bypass. In the EP laboratory, many steps are taken to avoid the inadvertent entrance of air, including tightening stopcock connections, de-airing tubing, proper preparation of manifolds, and the use of air filters along flush lines. A quick look at the spaghetti-like loops of flush tubing on the procedural field during a complex catheter ablation procedure makes it easy to understand how errors can occur that allow air to enter the systemic circulation (Figure 1).
A well-known complication of cardiac procedures and cardiac surgery is air embolism. Air in the systemic circulation can embolize into the cerebral and coronary arteries. In the OR, de-airing techniques are critical to safe cardiopulmonary bypass. In the EP laboratory, many steps are taken to avoid the inadvertent entrance of air, including tightening stopcock connections, de-airing tubing, proper preparation of manifolds, and the use of air filters along flush lines. A quick look at the spaghetti-like loops of flush tubing on the procedural field during a complex catheter ablation procedure makes it easy to understand how errors can occur that allow air to enter the systemic circulation (Figure 1).In addition to large air emboli, there has been interest in minimizing asymptomatic cerebral emboli (ACE) as seen on diffusion-weighted MR imaging scans after AF ablation procedures.1 Purported sources of ACE include clots on the sheaths and catheters in the left atrium, char that forms on overheated ablation tip electrodes, and microbubbles of gas that form when blood boils. Not all ablation technologies have the same risk of ACE. Indeed, gas formation leading to ACE limited the development of the non-irrigated multielectrode duty-cycled radiofrequency ablation catheters (Medtronic Ablation Frontiers).2 The cryoballoon system may have a lower rate of ACE compared to radiofrequency. Although it is debatable how important clinically these lesions are, it seems reasonable to avoid them if possible.
Another potential source of air embolism is inadvertent entry of air that is attached to or trapped within a device that is being deployed percutaneously into the heart. Avoiding this potential source of air is of rising importance, as the size of the transseptal sheaths is increasing with newer therapeutic devices that require larger transseptal sheaths, such as the cryoballoon, percutaneous mitral valve clips, and the percutaneous left ventricular assist device requiring left atrial placement.
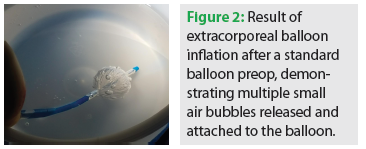 Tokuda et al recently published an interesting study that highlights the importance of optimally preparing devices before deployment to avoid air embolism.3 Currently, the cryoballoon is routinely prepped by carefully flushing the cryoballoon catheter lumen before and after placement of the circular pulmonary vein mapping catheter, and then placing the factory-wrapped balloon in a saline bath. In the bath, the protective introducer tube is pulled back and then replaced over the balloon to eliminate any air bubbles. Efforts are also made when entering the balloon catheter into the transseptal sheath to have a fluid-to-fluid interface at the time of entry. In some labs, the sheath is aspirated slightly to eliminate any air that might have come in through the diaphragm; in other labs, sheath entry is done with both parts submerged in a tray of saline. In this study, the investigators prepped the balloon in the saline bowl using standard techniques (with some additional massaging of the balloon to remove the air), but then also inflated the balloon under saline. Before the system will allow extracorporeal balloon inflation, the balloon has to be warmed to body temperature, which can be done by holding the balloon between one’s hands. They demonstrated that when the balloon is inflated, several small air bubbles are liberated from the crevices of the balloon and become attached to the balloon surface. Furthermore, Tokuda et al showed that there was a significant reduction in silent cerebral emboli seen on MRI of the brain 1-2 days after the ablation procedure. Reproduction of their observation is shown in Figure 2 and can be seen in the following video: https://www.youtube.com/watch?v=a_EMNAsWiOI
Tokuda et al recently published an interesting study that highlights the importance of optimally preparing devices before deployment to avoid air embolism.3 Currently, the cryoballoon is routinely prepped by carefully flushing the cryoballoon catheter lumen before and after placement of the circular pulmonary vein mapping catheter, and then placing the factory-wrapped balloon in a saline bath. In the bath, the protective introducer tube is pulled back and then replaced over the balloon to eliminate any air bubbles. Efforts are also made when entering the balloon catheter into the transseptal sheath to have a fluid-to-fluid interface at the time of entry. In some labs, the sheath is aspirated slightly to eliminate any air that might have come in through the diaphragm; in other labs, sheath entry is done with both parts submerged in a tray of saline. In this study, the investigators prepped the balloon in the saline bowl using standard techniques (with some additional massaging of the balloon to remove the air), but then also inflated the balloon under saline. Before the system will allow extracorporeal balloon inflation, the balloon has to be warmed to body temperature, which can be done by holding the balloon between one’s hands. They demonstrated that when the balloon is inflated, several small air bubbles are liberated from the crevices of the balloon and become attached to the balloon surface. Furthermore, Tokuda et al showed that there was a significant reduction in silent cerebral emboli seen on MRI of the brain 1-2 days after the ablation procedure. Reproduction of their observation is shown in Figure 2 and can be seen in the following video: https://www.youtube.com/watch?v=a_EMNAsWiOIPrevention of air embolism is critical during EP procedures. The study by Tokuda and colleagues has taught us how important it is to properly prepare devices before introducing them into the heart to eliminate all potential sources of trapped air. This is a good lesson for electrophysiologists and for the manufacturers of medical devices.
References
- Gaita F, Caponi D, Pianelli M, et al. Radiofrequency catheter ablation of atrial fibrillation: a cause of silent thromboembolism? Magnetic resonance imaging assessment of cerebral thromboembolism in patients undergoing ablation of atrial fibrillation. Circulation. 2010;122:1667-1673.
- Verma A, Debruyne P, Nardi S, et al. Evaluation and reduction of asymptomatic cerebral embolism in ablation of atrial fibrillation, but high prevalence of chronic silent infarction: results of the Evaluation of Reduction of Asymptomatic Cerebral Embolism Trial. Circ Arrhythm Electrophysiol. 2013;6:835-842.
- Tokuda M, Matsuo S, Kato M, et al. Effect of air removal with extracorporeal balloon inflation on incidence of asymptomatic cerebral embolism during cryoballoon ablation of atrial fibrillation. Heart Rhythm. 2017;14:1291-1296.

Current Issue
January 2025
Volume 25
Issue 1
Stay in the know.
EP Lab Digest Newsletter
