

Single-Center Experience of Utilizing App-Based Home Monitoring for Pacemaker and CRT-P Patients
“There is an app for that”™. –Trademarked by Apple in 2010
On June 29th, 2007, Apple, Inc. released the first touchscreen smartphone. Approximately one year later, Google followed suit with the release of the Android smartphone. In today’s society, the smartphone almost seems ubiquitous. According to Pew Research, 64% of adults in the United States own a smartphone of some kind — this is up from 35% in 2011.1 Smartphones have created an increase in the conveniences of services such as shopping, dating, and transportation.

This technology has also led to the development of new software applications for providing healthcare services, aiding physicians in healthcare information management and patient management, among other benefits.2 A study at Stanford University assessing the feasibility of using an app to measure and study cardiovascular health found that it was possible to use remote technology to get clinically relevant and detailed assessments of physical activity, fitness, and sleep.3

In 2001, BIOTRONIK received FDA approval for CardioMessenger, the first pacemaker/ICD remote monitor. Medtronic followed suit in 2005 with the CareLink Network, St. Jude Medical (now Abbott) with the Merlin@home™ Transmitter in 2008, and Boston Scientific with LATITUDE™ Home Monitoring System in 2009.4 The advantages for clinicians and patients have been immense. One study showed usage of remote monitoring in clinical practice was associated with a 30% reduction in hospitalization costs, 9810 fewer hospitalizations, 119,000 fewer days spent in hospital, and hospital payment savings of $370,270,000.5 Previous (and some current) generation home monitoring systems have relied on a standard analog telephone “landline” connection in order to securely send data. However, these landlines are rapidly becoming obsolete, with consumers discontinuing them at a rate of 700,000 landlines a month. In 2014, it was estimated that 41% of Americans do not use a landline.6 In response, companies have been transitioning to cellular and WiFi-based transmission of remote monitoring data. This has required partnering with device clinics to help clinics upgrade the old technology by providing cellular or internet router adapters. (Figure 1)
 In 2015, Medtronic became the first company to release an app-based monitor, the MyCareLink Smart, for both the Android and Apple platforms. The home monitor, a handheld device, utilizes either a cell phone or a tablet with an app to transmit the data from pacemakers securely to the remote monitoring servers (Figure 2). The app displays step-by-step instructions of how to do a transmission with the monitor (Figure 3). Here at the NYU Langone Heart Rhythm Center (HRC), while aiding our patients in upgrading their home monitors, we were finding that patients and their families were having difficulty using the WireX cellular adapter for use with the old analog-based CareLink 2490 Home Monitor. We saw this as an opportunity to consider a different approach for our pacemaker patients. Deciding to capitalize on the trend of smartphones, we began implementing the MyCareLink Smart. Below are four examples of use at the NYU Langone Heart Rhythm Center.
In 2015, Medtronic became the first company to release an app-based monitor, the MyCareLink Smart, for both the Android and Apple platforms. The home monitor, a handheld device, utilizes either a cell phone or a tablet with an app to transmit the data from pacemakers securely to the remote monitoring servers (Figure 2). The app displays step-by-step instructions of how to do a transmission with the monitor (Figure 3). Here at the NYU Langone Heart Rhythm Center (HRC), while aiding our patients in upgrading their home monitors, we were finding that patients and their families were having difficulty using the WireX cellular adapter for use with the old analog-based CareLink 2490 Home Monitor. We saw this as an opportunity to consider a different approach for our pacemaker patients. Deciding to capitalize on the trend of smartphones, we began implementing the MyCareLink Smart. Below are four examples of use at the NYU Langone Heart Rhythm Center.
Case 1: An 89-year-old female with Alzheimer’s disease.
The patient had a biventricular pacemaker implanted in 2007 due to advanced heart failure and complete AV block. The patient also has Alzheimer’s disease and was living in the care of her daughter. When attempting to do remote transmissions, she often ran into difficulty with error lights that kept flashing. This often led to missed transmissions due to the frustration of troubleshooting the monitor. However, the daughter and grandson both had a smartphone, and were quite capable of downloading and using an app. Once the MyCareLink Smart system was provided to the family, the transmissions began and have continued without any difficulty. 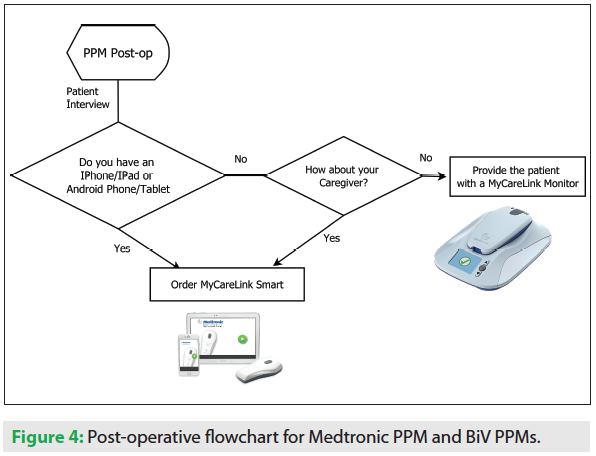
Case 2: A 55-year-old male who only speaks Tagalog.
The patient had a dual-chamber pacemaker implanted for sick sinus syndrome. The patient’s wife often managed his remote transmission appointments, since she speaks English. As in the previous case, the 2490 monitor was used over a landline, often resulting in a failed transmission. The patient’s wife had a smartphone, and was able to set it up to do a transmission with the app and the MyCareLink Smart system. This process, which previously took up to an hour for the patient, now takes only 10 minutes at most.
Case 3: A 33-year-old female pre-school teacher.
The patient was implanted with a dual-chamber pacemaker for cardiac sarcoidosis-induced complete AV block. The patient had a 24950 monitor, which she could use quite easily. One day at work, she felt her heart racing and associated shortness of breath. She did not feel it warranted an emergency room visit, but found that she would not be able to transmit until she got home later that day. She was brought in for an in-office evaluation to evaluate for possible arrhythmias. The device had logged false episodes of atrial tachycardia due to exercise, as well as some true atrial arrhythmias. Given her age, she was asked about having the MyCareLink Smart as an option. She would be able to keep it in her purse to have it with her the next time she felt symptoms. She readily agreed, and had no problem with the setup. Now when she has symptoms, she has the option to immediately do a transmission, allowing for rapid diagnosis and management.
Case 4: A 71-year-old male who was recently given a smartphone as a gift from his son.
The patient had a dual-chamber pacemaker implanted for bradycardia-tachycardia syndrome. Remote monitoring was important to assess his atrial arrhythmia burden following prior AT/AF ablations. However, by the patient’s own admission, he was not “technically savvy”. He often had difficulties with his landline-based remote monitor, and chose (more often than not) to come for in-person device evaluations as opposed to being monitored remotely. When presented with the idea of an MyCareLink Smart system that would work with his new smartphone, he was very reluctant, given his anxiety toward the use of technology. After some discussion, he finally agreed to try it out. Initially, setting up the monitor with him was difficult. The patient had forgotten his iTunes password, which was required to download the app. Even after he located the password, he called in, wondering what his “login” was to the MyCareLink Smart system. We realized he had downloaded the clinician app. He then successfully downloaded the patient app, doing it on his own without his son. When calling to express his joy at the new system working, he exclaimed “I am now a techie!” The staff here at HRC are very proud of him.
From these examples, the staff at NYU HRC Langone have found a way to use new technology to ease patient stress with home monitoring, while keeping up with the trends of mobile-based health technology. We also found that this tool could be used to address language barriers that may prevent a patient from enrolling in remote monitoring. From our examples and experiences in implementing the technology, our current screening process occurs during the post-operative appointment for new pacemaker implants (Figure 4). We constantly look for ways to integrate new technologies into our practice. Given that more than half of the U.S. population has a smartphone of some kind, it was inevitable that cardiac implantable electronic devices would be a part of mobile application health technologies. By working with patients to aid and integrate these technologies, we can improve healthcare outcomes, save healthcare dollars, and ease overall workflow for the clinic.
Disclosures: The authors of this paper received no compensation for writing this. Harish Duraiswami is a Cardiac Devices Specialist at NYU HRC; prior to that, he worked as a Clinical Specialist for Medtronic. Jane Smyth-Melsky has served as a consultant to Medtronic. Dr. Love serves as a consultant to Abbott, Medtronic, and Spectranetics; he is a member of the medical advisory board at Medtronic. Dr. Chinitz serves as a consultant to Abbott, BIOTRONIK, and Medtronic, and receives fellowship support from BIOTRONIK, Boston Scientific, and Medtronic.
References
- Smith A. U.S. Smartphone Use in 2015. Pew Research Center: Internet, Science & Tech. Published April 1, 2015. Available online at https://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015/. Accessed January 18, 2017.
- Ventola CL. Mobile Devices and Apps for Health Care Professionals: Uses and Benefits. PT. 2014;39(5):356-364.
- McConnell MV, Shcherbina A, Pavlovic A, et al. Feasibility of Obtaining Measures of Lifestyle From a Smartphone App: The MyHeart Counts Cardiovascular Health Study. JAMA Cardiol. 2017;2(1):67-76.
- Burri H, Senouf D. Remote monitoring and follow-up of pacemakers and implantable cardioverter defibrillators. Europace. 2009;11(6):701-709.
- Piccini JP, Mittal S, Snell J, Prillinger JB, Dalal N, Varma N. Impact of remote monitoring on clinical events and associated health care utilization: A nationwide assessment. Heart Rhythm. 2016;13(12):2279-2286.
- Cutting the cord. The Economist. Published August 15, 2009. Available online at https://www.economist.com/node/14214847. Accessed January 18, 2017.
- MyCareLink Smart US. (n.d.). Retrieved April 17, 2017, from https://play.google.com/store/myplayactivity?hl=en, Medtronic Inc. Google Play.

