

Shifting Paradigms: A New Comprehensive Multi-Disciplinary Approach to Atrial Fibrillation
While atrial fibrillation is one of the most common heart rhythm disorders in the world, affecting more than five million people in the U.S., it is also one of the more challenging conditions to treat, particularly for patients with persistent or permanent atrial fibrillation.1 Patients with persistent or longstanding permanent atrial fibrillation and enlarged atria have not historically been good candidates for conventional catheter treatment as results have been limited. Surgical approaches have historically been more invasive, have a higher adverse event rate, and are only moderately effective when compared to percutaneous catheter ablation.2
Two Disciplines, One Procedure
Our center has evaluated and adopted a multidisciplinary approach drawing on the expertise of the electrophysiologist and cardiothoracic surgeon for treatment of atrial fibrillation, and the results to date have been promising. The convergent procedure is a minimally invasive, epicardial approach that provides complete, visible cardiac access without chest incisions or ports, lung deflation, or pericardial dissections. During the first part of the procedure, the surgeon creates a linear lesion pattern on a beating heart under direct endoscopic visibility. Next, the EP utilizes endocardial mapping and ablation to create and confirm isolation of the pulmonary veins and the posterior left atrium.
To date, our center has performed over 180 of these cases, and the multidisciplinary approach has demonstrated strong single-procedure efficacy and an excellent safety profile. This approach may represent a paradigm shift in the treatment of atrial fibrillation and has the potential to transform the way EPs treat persistent patients. While close collaboration and coordination with a surgeon is not commonplace in arrhythmia management, the partnership has proven invaluable and should be a part of every electrophysiologist’s tool bag. In fact, together we have been more effective than we were working independently, and we continue to collaborate to evolve and improve our techniques.
Clinical Experience with Convergent Procedure
Approximately 184 patients have been treated thus far with the convergent procedure. Most of these patients have symptomatic persistent or longstanding permanent atrial fibrillation, although some patients with paroxysmal atrial fibrillation with enlarged atria have been included.
The primary clinical advantage of the convergent procedure is in the ability to provide a truly minimally invasive option that is comprehensive and predictive of outcomes, while potentially improving safety. The combined approach is performed in a single setting, the EP lab, and offers an effective new treatment for those patients who historically have not been considered ideal candidates for catheter ablation. The procedure begins through a single, small incision in the abdomen (2.5 cm) to create a subxyphoid pericardial window, which provides the surgeon access 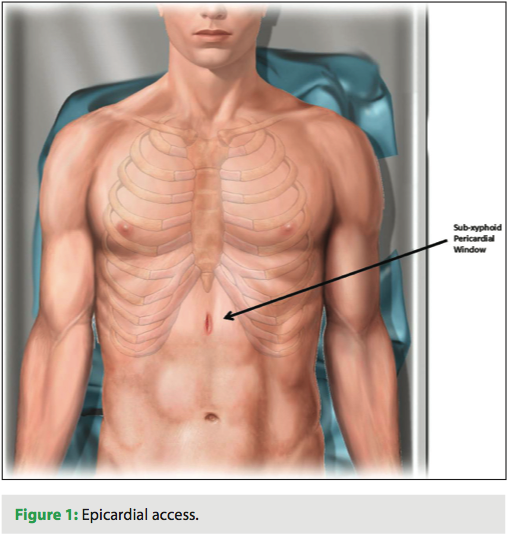 to the posterior left atrium and pulmonary veins (Figure 1). The surgeon then creates a comprehensive pattern of long, linear lesions under direct endoscopic visualization on a beating heart (Figures 2 and 3). The advantage for me, as an EP, is that the entire posterior left atrium can be isolated safely through epicardial ablation, thus minimizing the risk of collateral tissue damage. Once the epicardial portion is complete, the EP uses a Lasso catheter to diagnostically confirm pulmonary vein entrance and exit block, ablate endocardially to complete
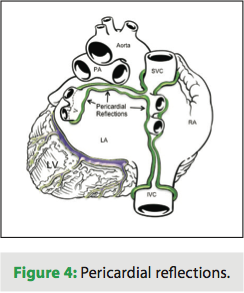
to the posterior left atrium and pulmonary veins (Figure 1). The surgeon then creates a comprehensive pattern of long, linear lesions under direct endoscopic visualization on a beating heart (Figures 2 and 3). The advantage for me, as an EP, is that the entire posterior left atrium can be isolated safely through epicardial ablation, thus minimizing the risk of collateral tissue damage. Once the epicardial portion is complete, the EP uses a Lasso catheter to diagnostically confirm pulmonary vein entrance and exit block, ablate endocardially to complete 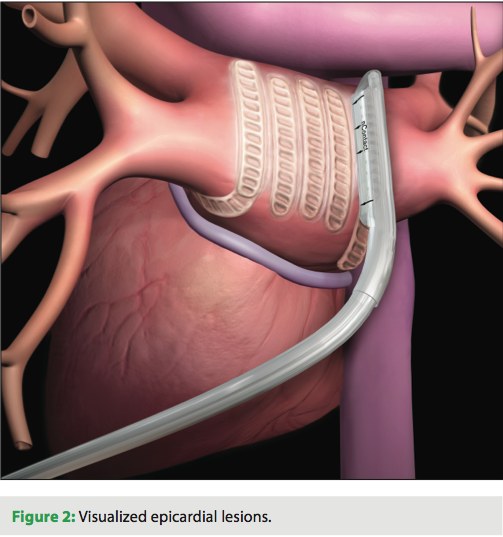 the lesion pattern, and performs a cavotricuspid isthmus line. Most gaps in the epicardial ablation can be found by the electrophysiologist at the pericardial reflections (Figure 4). The combined approach is more comprehensive and utilizes checks and balances by allowing the EP to check for block and scar following epicardial ablation (Figure 5).
the lesion pattern, and performs a cavotricuspid isthmus line. Most gaps in the epicardial ablation can be found by the electrophysiologist at the pericardial reflections (Figure 4). The combined approach is more comprehensive and utilizes checks and balances by allowing the EP to check for block and scar following epicardial ablation (Figure 5).
 Most patients remain in the hospital for monitoring for three days after the procedure. Follow-up monitoring focuses on EKG at one month and three months and with any symptoms. A 14-day event monitor is placed at six months, 12 months, and annually thereafter. Most patients remain on antiarrhythmic medications for eight to 12 weeks post procedure, and then medications are discontinued.
Most patients remain in the hospital for monitoring for three days after the procedure. Follow-up monitoring focuses on EKG at one month and three months and with any symptoms. A 14-day event monitor is placed at six months, 12 months, and annually thereafter. Most patients remain on antiarrhythmic medications for eight to 12 weeks post procedure, and then medications are discontinued.
Overall Results to Date
 Using the convergent procedure instead of a stand-alone percutaneous catheter approach has allowed us to obtain a higher success rate in relieving more complex atrial fibrillation patients. Particularly among those patients with persistent or longstanding permanent atrial fibrillation, early evidence shows that success rates with the convergent procedure are superior to our results with catheter ablation, and are not dependent on multiple procedures to gain the desired result.
Using the convergent procedure instead of a stand-alone percutaneous catheter approach has allowed us to obtain a higher success rate in relieving more complex atrial fibrillation patients. Particularly among those patients with persistent or longstanding permanent atrial fibrillation, early evidence shows that success rates with the convergent procedure are superior to our results with catheter ablation, and are not dependent on multiple procedures to gain the desired result.
 Data presented from our center during the Heart Rhythm Society meeting in May 2012 demonstrated successful outcomes in patients with drug refractory or intolerant persistent or longstanding permanent atrial fibrillation as well as selected patients with paroxysmal atrial fibrillation (n=104).3 The average patient age was 60.9 years with an average duration of 5.2 years of atrial fibrillation. In that study, patients underwent the convergent procedure and had follow-up at one, three, six and 12 months.
Data presented from our center during the Heart Rhythm Society meeting in May 2012 demonstrated successful outcomes in patients with drug refractory or intolerant persistent or longstanding permanent atrial fibrillation as well as selected patients with paroxysmal atrial fibrillation (n=104).3 The average patient age was 60.9 years with an average duration of 5.2 years of atrial fibrillation. In that study, patients underwent the convergent procedure and had follow-up at one, three, six and 12 months.
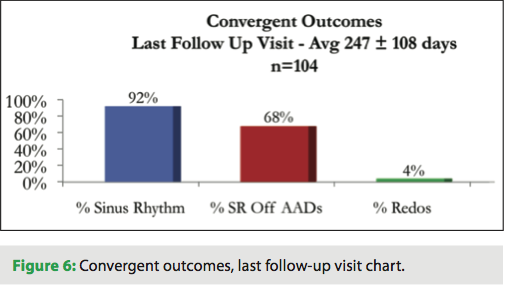 At one-year follow-up, 81% of patients in the study were in sinus rhythm and 69% were in sinus rhythm off of antiarrhythmic medications. At last follow up, 92% of patients were in sinus rhythm and 68% were in sinus rhythm off of antiarrhythmic medications. The consistency of the data over time and the low redo rate make the procedure an attractive treatment alternative.
At one-year follow-up, 81% of patients in the study were in sinus rhythm and 69% were in sinus rhythm off of antiarrhythmic medications. At last follow up, 92% of patients were in sinus rhythm and 68% were in sinus rhythm off of antiarrhythmic medications. The consistency of the data over time and the low redo rate make the procedure an attractive treatment alternative.
Importantly, there has been no noted increase in complications related to the procedure’s increased efficacy. In the HRS study presented earlier this year, there were no major adverse cardiac events reported less than 30 days after surgery. We also observed a low rate of major adverse cardiac events after 30 days post-op, including one stroke in a patient who had severe LV dysfunction and one transient ischemic attack.
Discussion: Utilizing Innovation to Create New Programs
We are entering a new day in healthcare where proving safety and efficacy for new devices and procedures is not enough; we also need to meet evidenced-based, quality metrics and demonstrate that healthcare dollars are justified through cost benefit savings to the system. As we consider the convergent procedure, there appear to be significant cost benefits. We are talking about a broader, more persistent patient population with higher morbidity and mortality rates, and consequentially, higher burden to the healthcare system. However, the patient population is growing rapidly.
EPs are going to have to adopt new innovative approaches and consider how we apply lessons from the Centers for Excellence model that can deliver more comprehensive treatment alternatives to a broader group of arrhythmia patients.
Conclusion
With the incidence of atrial fibrillation on the rise and managed care demanding greater cost savings, we have an obligation to patients and payers to evaluate new treatment options. Innovation has always driven medical progress by forging new pathways and improvements in patient outcomes across a myriad of disease states.
Our center is actively engaged in evaluating innovation that improves patient outcomes, identifying new patient segments likely to benefit from novel approaches, and helping evolve and improve new techniques. The convergent method has become a cornerstone of our atrial fibrillation program because it is a tool from which we can leverage our existing technologies and experience to expand our capabilities, effectively reaching the broader atrial fibrillation patient population, and helping to meet both the demands of patients and the healthcare system.
Disclosures: Dr. Civello reports that his institution has received a grant from the Cardiovascular Research Foundation of Louisiana for data collection, and that he has received a consulting fee for education of visiting physicians. He also reports receiving travel accommodations for a clinical advisory meeting.
References
- Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119–125.
- Han FT, Kasirajan V, Kowalski M, et al. Results of a minimally invasive surgical pulmonary vein isolation and ganglionic plexi ablation for atrial fibrillation: Single-center experience with 12-month follow-up. Circ Arrhythm Electrophysiol 2009;2:370–377.
- Combined Epicardial and Endocardial Ablation for Atrial Fibrillation: Single Center Experience in 100 Consecutive Patients. Oral Presentation at the May 2012 Heart Rhythm Society Meeting.

