

Cover Story
Remote Monitoring of Heart Failure: A Single-Center Experience
In this interview, Jonathan Rosman, MD, FACC, FHRS talks about his approach to remote monitoring of congestive heart failure (CHF).
Tell us about your practice.
 I joined Cardiac Arrhythmia Service, located in South Florida, after completing my EP fellowship 6 years ago at Brigham and Women’s Hospital. I have 2 partners, Dr. Murray Rosenbaum and Dr. Martin Kloosterman. We also have 2 physician assistants. We have a research coordinator and are involved in clinical studies. Our practice is limited to electrophysiology, and we have a large referral network from general cardiologists in the area.
I joined Cardiac Arrhythmia Service, located in South Florida, after completing my EP fellowship 6 years ago at Brigham and Women’s Hospital. I have 2 partners, Dr. Murray Rosenbaum and Dr. Martin Kloosterman. We also have 2 physician assistants. We have a research coordinator and are involved in clinical studies. Our practice is limited to electrophysiology, and we have a large referral network from general cardiologists in the area.
We lecture at the College of Medicine at Florida Atlantic University (FAU), and teach EKGs and electrophysiology to FAU residents. Our practice is affiliated with 3 hospitals: Boca Raton Regional Hospital, Delray Medical Center, and West Boca Medical Center.
We perform complex ablations, including for atrial fibrillation and ventricular tachycardia. We routinely perform fluoroless ablation for SVT, atrial flutter, and atrial fibrillation. Thanks to a generous donation from our patient, we were the third site in the U.S. to obtain the CardioInsight™ Noninvasive 3D Mapping System (Medtronic). Dr. Rosenbaum is the largest volume operator of CardioInsight in the U.S. We also perform all types of device implantations, including subcutaneous ICDs, leadless pacemakers, and direct His bundle pacing. We have a very active cardiac device remote monitoring service with over 2,000 patients. Dr. Kloosterman has pioneered the use of remote monitoring in the hospital setting. We are the largest users of CareLink Express (Medtronic) in the country.
Why is remote monitoring important?
 Remote monitoring is associated with a morbidity and mortality benefit for patients with pacemakers and defibrillators.1-3 By monitoring patients on a daily basis, we are able to immediately diagnose and treat arrhythmias and device/lead-related problems. If we discover atrial fibrillation, we start the patient on anticoagulation right away, then have them follow up in our office or with their cardiologist. If we find a ventricular arrhythmia, we start antiarrhythmic medications over the phone or admit the patient to the hospital to prevent recurrent VT and ICD shocks. If we see lead- or device-related issues, we immediately arrange appropriate care to prevent inappropriate ICD shocks or loss of pacemaker function. Remote monitoring has revolutionized the practice of cardiac electrophysiology and has markedly improved patient outcomes.1-2
Remote monitoring is associated with a morbidity and mortality benefit for patients with pacemakers and defibrillators.1-3 By monitoring patients on a daily basis, we are able to immediately diagnose and treat arrhythmias and device/lead-related problems. If we discover atrial fibrillation, we start the patient on anticoagulation right away, then have them follow up in our office or with their cardiologist. If we find a ventricular arrhythmia, we start antiarrhythmic medications over the phone or admit the patient to the hospital to prevent recurrent VT and ICD shocks. If we see lead- or device-related issues, we immediately arrange appropriate care to prevent inappropriate ICD shocks or loss of pacemaker function. Remote monitoring has revolutionized the practice of cardiac electrophysiology and has markedly improved patient outcomes.1-2How have you incorporated remote monitoring into your practice?
 Remote monitoring maximizes our group’s efficiency. We can manage and treat more patients by reducing the number of in-office visits needed for patients followed remotely. We currently remotely monitor 850 patients with implantable defibrillators, 750 patients with implantable loop recorders, and 400 patients with pacemakers. We also have 300 patients in our remote heart failure monitoring program. We have 2 technicians who download and review transmissions on a daily basis. Transmissions that require review are evaluated by a physician, and after a plan of care has been established, the transmission and note are scanned into the EMR. A physician or physician assistant will contact the patient by phone to review the information and plan of care. We are a team of secretaries, technicians, nurses, physician assistants, and physicians all working together to optimize patient care for our remote monitoring program.
Remote monitoring maximizes our group’s efficiency. We can manage and treat more patients by reducing the number of in-office visits needed for patients followed remotely. We currently remotely monitor 850 patients with implantable defibrillators, 750 patients with implantable loop recorders, and 400 patients with pacemakers. We also have 300 patients in our remote heart failure monitoring program. We have 2 technicians who download and review transmissions on a daily basis. Transmissions that require review are evaluated by a physician, and after a plan of care has been established, the transmission and note are scanned into the EMR. A physician or physician assistant will contact the patient by phone to review the information and plan of care. We are a team of secretaries, technicians, nurses, physician assistants, and physicians all working together to optimize patient care for our remote monitoring program.We also use remote monitoring in the hospital setting. Instead of waiting for a device representative or physician to check a patient’s device, the nurse is able to send a remote transmission, which we can instantly access for evaluation. Remote transmission for all post-op device patients are done by the night shift nurse, and the report is available in the chart by 7am. The ER also performs remote transmissions for all their device checks. We are able to immediately access and review these transmissions, allowing for timely and efficient patient care.
Describe remote monitoring for heart failure.
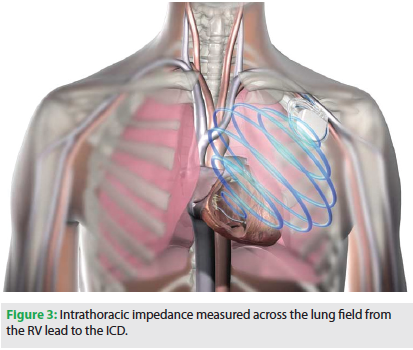
 Implantable defibrillators can monitor intrathoracic impedance. The lungs are located between the RV lead and defibrillator, and by measuring the resistance between them, the defibrillator can assess pulmonary fluid status. Conduction is faster through water; therefore, lower intrathoracic impedance (lower resistance) suggests pulmonary fluid accumulation. Low intrathoracic impedance values precede clinical signs and symptoms of congestive heart failure.4-5 Studies show that patients with low intrathoracic impedance measurements are at increased near-term risk of CHF hospitalization.4-6 By remotely monitoring changes in intrathoracic impedance, we can potentially prevent heart failure exacerbations and hospitalizations.
Implantable defibrillators can monitor intrathoracic impedance. The lungs are located between the RV lead and defibrillator, and by measuring the resistance between them, the defibrillator can assess pulmonary fluid status. Conduction is faster through water; therefore, lower intrathoracic impedance (lower resistance) suggests pulmonary fluid accumulation. Low intrathoracic impedance values precede clinical signs and symptoms of congestive heart failure.4-5 Studies show that patients with low intrathoracic impedance measurements are at increased near-term risk of CHF hospitalization.4-6 By remotely monitoring changes in intrathoracic impedance, we can potentially prevent heart failure exacerbations and hospitalizations.Have studies demonstrated a clinical benefit for heart failure monitoring?
 Studies have consistently demonstrated the predictive nature of low intrathoracic impedance and the increased risk of CHF exacerbation and hospitalization.6-7 However, the utilization of this data to improve clinical outcomes is not well established.8 The DOT-HF study evaluated whether intrathoracic impedance values could be utilized to decrease hospitalizations.9 Patients received an audible alert to a decrease in intrathoracic impedance. Results showed an increase in hospitalizations in the treatment group compared with the control group. However, the presence of an audible alert and the lack of remote monitoring may have impacted these results. Heart failure treatment and hospitalizations in DOT-HF were often driven by the audible alert, even in the absence of clinical symptoms. Similarly, the LIMIT-CHF study studied the presence of an audible alert to low intrathoracic impedance to reduce CHF hospitalizations.10 Every patient with an audible alert was instructed to increase their diuretic dose for a week. There was no difference in outcome between the two groups. However, patients were treated solely based on an alert, even in the absence of clinical symptoms.
Studies have consistently demonstrated the predictive nature of low intrathoracic impedance and the increased risk of CHF exacerbation and hospitalization.6-7 However, the utilization of this data to improve clinical outcomes is not well established.8 The DOT-HF study evaluated whether intrathoracic impedance values could be utilized to decrease hospitalizations.9 Patients received an audible alert to a decrease in intrathoracic impedance. Results showed an increase in hospitalizations in the treatment group compared with the control group. However, the presence of an audible alert and the lack of remote monitoring may have impacted these results. Heart failure treatment and hospitalizations in DOT-HF were often driven by the audible alert, even in the absence of clinical symptoms. Similarly, the LIMIT-CHF study studied the presence of an audible alert to low intrathoracic impedance to reduce CHF hospitalizations.10 Every patient with an audible alert was instructed to increase their diuretic dose for a week. There was no difference in outcome between the two groups. However, patients were treated solely based on an alert, even in the absence of clinical symptoms. How does your approach differ from prior studies?
When treating patients with congestive heart failure, it is imperative to involve the patient. Prior studies have focused primarily on intrathoracic impedance measurements rather than patients and their symptoms. In LIMIT-CHF, patients were treated with diuretics irrespective of clinical symptoms.10 In DOT-HF, every patient alert had to be treated until the intrathoracic impedance normalized, even in the absence of symptoms.9 This likely led to overtreatment and unnecessary hospitalizations.
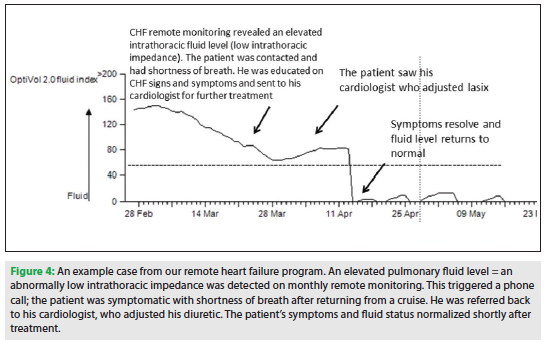
Intrathoracic impedance is an early marker of increased pulmonary fluid levels. However, the body self-adjusts and intrathoracic impedance levels often normalize without any intervention. Therefore, we sought to use a low intrathoracic impedance value as a screening tool rather than an indication to treat. We utilize a patient-centered educational approach to abnormal intrathoracic impedance values. With monthly remote evaluation of patients’ intrathoracic impedance, we are able to detect patients who are at higher risk of hospitalization. All patients with low intrathoracic impedance are contacted by a nurse, physician, or physician assistant. The health care professional assesses the patient, and then educates them on signs and symptoms of heart failure. Only patients who are symptomatic are sent to their cardiologists for further evaluation and treatment. This minimizes overtreatment and, at the same time, empowers patients to participate in their medical care. With our approach, we have an extremely low rate of heart failure hospitalizations.11
How do patients and cardiologists feel about your approach to remote heart failure monitoring?
We work together with our referring cardiologists to provide the best care for our patients. Since we only practice electrophysiology, we refer all of our symptomatic heart failure patients back to their cardiologist for further treatment. Our patients appreciate the close monitoring and follow-up that we provide. We do a follow-up phone call the month after we detect an abnormal intrathoracic impedance, to ensure the patient is doing well and was not hospitalized. By involving our patients in their treatment, they feel more responsible for their medical care. Our patient-centered educational approach to remote heart failure monitoring is unique, effective, and can reduce heart failure exacerbations and hospitalizations.
Disclosures: The author has no conflicts of interest to report regarding the content herein.
References
- Mittal S, Piccini JP, Snell J, et al. Improved survival in patients enrolled promptly into remote monitoring following cardiac implantable electronic device implantation. J Interv Card Electrophysiol. 2016;10:1-8.
- Landolina M, Perego GB, Lunati M, et al. Remote monitoring reduces healthcare use and improves quality of care in heart failure patients with implantable defibrillators: the evolution of management strategies of heart failure patients with implantable defibrillators (EVOLVO) study. Circulation. 2012;125(24):2985-2992.
- Slotwiner D, Varma N, Akar JG, et al. HRS Expert Consensus Statement on remote interrogation and monitoring for cardiovascular electronic implantable devices. Heart Rhythm. 2015;12(17)e69-e100.
- Cowie MR, Sarkar S, Koehler J, et al. Development and validation of an integrated diagnostic algorithm derived from parameters monitored in implantable devices for identifying patients at risk for heart failure hospitalization in an ambulatory setting. Eur Heart J. 2013;34(31):2472-2480.
- Yu CM, Wang L, Chau E, et al. Intrathoracic impedance monitoring in patients with heart failure correlation with fluid status and feasibility of early warning preceding hospitalization. Circulation. 2005;112(6):841-848.
- Small RS, Wickemeyer W, Germany R, et al. Changes in intrathoracic impedance are associated with subsequent risk of hospitalizations for acute decompensated heart failure: clinical utility of implanted device monitoring without a patient alert. J Card Fail. 2009;15(6):475-481.
- Whellan DJ, Ousdigian KT, Al-Khatib SM, et al. Combined heart failure device diagnostics identify patients at higher risk of subsequent heart failure hospitalizations: results from PARTNERS HF (Program to Access and Review Trending Information and Evaluate Correlation to Symptoms in Patients With Heart Failure) study. J Am Coll Cardiol. 2010;55(17):1803-1810.
- Van Veldhuisen DJ, Maass AH. Telemonitoring of outpatients with heart failure: a search for the holy grail? Circulation. 2012;125:2965-2967.
- Van Veldhuisen DJ, Braunschweig F, Conraads V, et al. Intrathoracic impedance monitoring, audible patient alerts, and outcome in patients with heart failure. Circulation. 2011;124(16):1719-1726.
- Domenichini G, Rahneva T, Diab IG, et al. The lung impedance monitoring in treatment of chronic heart failure (the LIMIT-CHF study). Europace. 2016;18(9):428-435.
- Rosman J, Rosenbaum M, Kloosterman EM. A Patient-centered Educational Approach To Intrathoracic Impedance Remote Monitoring Can Reduce Hospitalizations. J Inn Card Rhythm Man. 2016;7(10)296-249.

Current Issue
April 2025
Volume 24
Issue 4
Stay in the know.
EP Lab Digest Newsletter
