

Multidisciplinary Approach to Patient Care and Research in the Management of Stroke Patients
The Mass General Institute for Heart, Vascular and Stroke Care offers a novel approach to comprehensive, multispecialty clinical care to advance the diagnosis and treatment of cardiovascular and cerebrovascular diseases. By using this integrated approach, the Institute is pioneering a patient- and disease-focused care model that provides the best possible quality of care today while also discovering the medicine of tomorrow.
Launched in 2012, the Mass General Institute for Heart, Vascular and Stroke Care focuses on four key pillars that include integrated, personalized clinical care, a commitment to support novel clinical and translational research strategies for our world-class investigators, broad educational initiatives, and advocacy for quality care delivery and public policy leadership on the local, state and national stages. The Institute aims to improve the quality and value of patient care by fully utilizing a synergistic work environment built on clinical collaboration. With this foundation, the Institute plans to initiate integration of clinical care and research across disciplines.
four key pillars that include integrated, personalized clinical care, a commitment to support novel clinical and translational research strategies for our world-class investigators, broad educational initiatives, and advocacy for quality care delivery and public policy leadership on the local, state and national stages. The Institute aims to improve the quality and value of patient care by fully utilizing a synergistic work environment built on clinical collaboration. With this foundation, the Institute plans to initiate integration of clinical care and research across disciplines.
A critical component of the Institute is our world-class Stroke Service. Led by nationally renowned stroke neurologist Lee Schwamm, MD, the MGH Stroke Service offers an acute stroke response team and all facets of cerebrovascular care. These include a state-of-the-art Neurosciences Intensive Care Unit and a multispecialty Neuroendovascular program composed of neurovascular radiologists, neurosurgeons, and an interventional stroke neurologist.
The MGH Stroke Service runs an Acute Stroke Service with 24-hour a day coverage throughout the year. The acute stroke team consists of a dedicated stroke fellow (currently including a total of 11 board-certified and/or board-eligible neurologists at PGY 5 or 6 level), a neurology resident (PGY 2), and an acute stroke attending, of whom there are 12 staff vascular and critical care neurologists. The stroke fellow and neurology resident take calls in-house, guaranteeing that at least two members of the team are in the hospital at all times. The acute stroke team works closely with the MGH Emergency Department as a well-coordinated, multidisciplinary team that operates around the clock and is activated by a group paging system with notification of patient arrival. In addition to the acute stroke fellow, attending, and dedicated emergency neurology resident, the Emergency Department team is comprised of an emergency medicine senior, neurointerventional fellow and attending, neuroradiology fellow and attending, CT technician, and emergency pharmacist on call. Upon direct or estimated acute ischemic stroke patient arrival within 12 hours of stroke symptom onset, the team is activated by a service-wide page and prepared to execute the MGH acute stroke protocol. This protocol is geared to emergent evaluation of all acute ischemic stroke patients for potential therapeutic interventions or ongoing clinical trials around the clock. The Acute Stroke Service annually cares for more than 700 patients with acute ischemic stroke, as well as provides a year-round in-house consult service.
As the Chair of the Education Committee at the Institute, I also have the opportunity to collaborate with my cardiology and vascular colleagues both on the clinical as well as administrative level, as educational opportunities are built for multidisciplinary components of the Institute.
A Collaborative Approach to Patient Care
The Institute’s multidisciplinary approach has impacted patient care in addition to fostering a collaborative working environment. Many of us in the Department of Neurology have come to the realization that reaching out to our colleagues in different departments (e.g., Vascular Medicine, Cardiology and Radiology), to discuss patient cases and gather their expertise, benefits both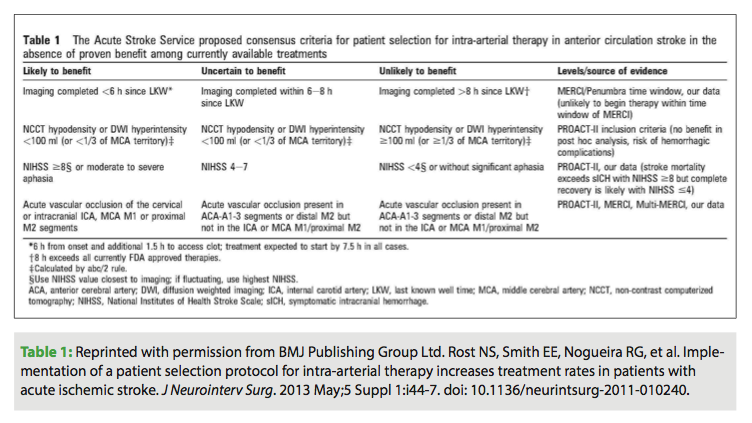 patients and providers by delivering a more comprehensive approach to care. Typically, there are perceived obstacles for crossing the barriers of administrative entities such as divisions and departments, but collaboration between departments has become apparent and visible. Treatment for patients with cerebrovascular and cardiovascular disease is very complex, and often, the opinions of multiple experts are necessary before a sensible management or patient diagnosis plan can be developed. This collaboration has already shown improvement in patient care.
patients and providers by delivering a more comprehensive approach to care. Typically, there are perceived obstacles for crossing the barriers of administrative entities such as divisions and departments, but collaboration between departments has become apparent and visible. Treatment for patients with cerebrovascular and cardiovascular disease is very complex, and often, the opinions of multiple experts are necessary before a sensible management or patient diagnosis plan can be developed. This collaboration has already shown improvement in patient care.
For instance, a great example of a collaborative environment at the Institute is our work on a multidisciplinary patent foramen ovale (PFO) committee, which consists of neurologists and cardiologists, as well as interventionalists, electrophysiologists, and hematologists. This defect is commonly linked to risk of stroke in young patients. PFO is typically an “incidental finding” when a patient presents with a cardiac condition; however, in young patients with otherwise unexplained cerebral ischemia, the potential role of PFO in etiology of stroke requires a thorough evaluation.
In August 2013 I treated a young patient who was a very active, previously healthy mother of two. She had experienced unusual symptoms that she did not know how to interpret. Neither the patient nor her husband realized she was having a stroke, and she presented to the hospital too late to be considered for acute interventions. Fortunately, her symptoms recovered quickly and in full, but in the process of etiologic stroke work-up, she was diagnosed with a PFO and decided to undergo a PFO closure. At the Institute, all stroke patients undergo a thorough underlying cause evaluation including a cardiac interrogation such as an echocardiogram, Holter monitoring or extended cardiac monitoring, and advanced imaging such as cardiac MRI. In this particular case, the patient was also found to have a genetic mutation that predisposed her to blood clotting. The array and complexity of medical issues in this case represented a classic example of a candidate who could greatly benefit from the expertise of the Institute’s multidisciplinary team. The Institute’s integrated approach allowed for the cardiologist’s involvement as well as generated a discussion with the Neurology team on whether this particular patient was a candidate for intervention. The hematologist also evaluated the patient to define the extent of her hypercoagulability status as a risk factor for future clotting. This collaboration between multiple colleagues and divisions allowed us to arrive at the treatment plan deemed to be most beneficial for this patient, and helped us individualize her care.
Another aspect of collaborative work at the Institute is the interface between Stroke Neurology and Cardiac Electrophysiology. We convene most frequently regarding the management of our most complicated cases of atrial fibrillation (AF), in patients who are not able to tolerate anticoagulation for secondary stroke prevention. These patients have usually experienced multiple cerebrovascular events, including ischemic and hemorrhagic stroke, and ultimately, their management options have been narrowed. A similar dilemma arises in patients with AF and, for example, a specific small cerebral vessel pathology such as cerebral amyloid angiopathy, which carries a high risk of primary hemorrhagic stroke. In these complex cases, we do not hesitate to reach out to our colleagues from Cardiac Electrophysiology to examine whether a heart procedure could be beneficial in controlling their rhythm in lieu of anticoagulants, with the purpose of lowering these patients’ risk of future stroke. Working with the electrophysiologists at the Institute has been instrumental in helping us treat these patients with co-existing conditions and improving overall patient outcomes.
Systematic Approach for Acute Stroke Therapies
Continuing on with the Institute’s collaborative mentality, we have spearheaded a team effort among neurologists, neurointerventionalists, Emergency Medicine physicians and neuroradiologists within the Institute to develop a systematic approach to patient selection for acute stroke therapies in order to optimize their outcomes.
Based on the developed criteria, the patient moves quickly along the diagnostic pathway, from the Emergency Department to neuroimaging area, where clot-busting medication is frequently administered for eligible patients, and decisions are made with regard to the further management options for patients with acute ischemic stroke based on the “likely to benefit” criteria (Table 1). Furthermore, we have been able to demonstrate that implementation of the patient selection protocol for intra-arterial therapy has increased treatment rates in patients with acute ischemic stroke.
The Future of the Institute
In addition to the Institute’s ongoing research collaborations, the Stroke Division at Mass General has recently been selected as one of the sites for the NINDS Stroke Trials Network, or NIH StrokeNET. As part of this large project grant, 25 academic stroke centers in the United States have received funding to develop a premiere network for clinical trials in stroke prevention, treatment and recovery.
The stroke research community has been lacking the pace and volume of large-scale trials that bring effective and safe treatments to patients. This new initiative by NINDS holds an extraordinary opportunity to increase general knowledge of stroke and other cerebrovascular disorders, improve patient care and make an impact on public health. Mass General, a central hub of the New England Regional Coordinating Center (NERCC) that is linked to the seven largest academic medical centers in the area as its spokes, will play an instrumental role in the NINDS Stroke Trials Network. The infrastructure that will be developed over the next five years will increase the research collaboration within the Institute and broaden its multidisciplinary expertise. We anticipate that future stroke clinical trials will allow greater involvement of our colleagues throughout the Institute and serve as a powerful example to other major academic centers.
These collaborations at the Institute will continue to nurture the development of cutting-edge research across divisions and departments to advance science and improve patient outcomes.
Disclosure: The author has no conflicts of interest to report regarding the content herein.
On-Demand Webcast
New Convergent Ablation Options for Managing Persistent Atrial Fibrillation
www.naccme.com/program/2013-574-1
Expiration date: June 30, 2014
This activity is designed for electrophysiologists, cardiothoracic surgeons, physicians in related specialties, and allied health professionals involved in the care of electrophysiology and cardiothoracic surgical patients including nurses, physician assistants, and perfusionists.
Supported by an educational grant from nContact, Inc. There is no fee associated with this activity.

