

Cover Story
From the Mercury Capillary Electrometer to the Wireless, Battery-Less Pacemaker: State-of-the-Art Innovations in the Treatment of Arrhythmia
In this article, we provide a brief review of the historical progression of cardiac electrophysiology as well as highlight recent developments in our research lab to advance the treatment of arrhythmia.
Background of Cardiac EP
Electrocardiogram
In 1887, Augustus Waller recorded the first human electrocardiogram (ECG) with a mercury capillary electrometer, which consisted of a single fine-draw glass tube that was filled with mercury and immersed in sulfuric acid.1 This instrument was capable of recording the body’s surface voltage changes on photographic paper, which was detected by moving the mercury in response to potential electrical changes.2
In 1889, at the first International Congress of Physiological Sciences in Basel, Switzerland, Willem Einthoven observed the recording of a human electrocardiogram with the capillary electrometer by Augustus Waller. This led Einthoven to begin his studies of the ECG with the mercury capillary electrometer.3 By the end of the nineteenth century, he was able to register good electrocardiographic representations with the mercury capillary electrometer through complex mathematical and physical approaches.3 Furthermore, in 1901, Einthoven further improved ECG recordings by devising the first direct recorder of the true human electrocardiogram by using a modified string galvanometer. This development helped electrocardiography become clinically relevant,2 and Einthoven moved on to define different arrhythmias such as bigeminy, atrial flutter and fibrillation, left and right ventricular hypertrophy, and the “P mitrale.”4
External cardiac pacemaker
In 1926, an Australian anesthesiologist named Mark Lidwill used an alternating current (AC) to stimulate a patient’s heart by inserting a needle into their ventricle. In 1932, American physiologist Albert Hyman invented a device that could drive a direct current (DC) into a patient’s right atrium via a bipolar needle electrode (inserted via an intercostal space).5
Pacemakers and internal defibrillators
In 1959, Rune Elmquist and Ake Senning reported the first successful implantation of an internal pacemaker, which led the way to the development of device therapy for managing arrhythmia.6 In 1970, the concept of the implantable cardioverter-defibrillator (ICD) was first published by Michel Mirowski, and in 1980, Mirowski and his colleagues implanted the first ICD in a patient.7
Atrial fibrillation (AF) catheter ablation
In the early 1990s, John Swartz paved the way for catheter ablation in the electrophysiology lab by attempting to replicate the Cox-Maze surgery concept, a surgical procedure to cure AF by making a maze-like pattern of incisions in the upper chambers of the heart. A high rate of complications, long fluoroscopy time, and a very lengthy procedure made Swartz’s experiments too futile to be continued.8 Then in 1998, a groundbreaking breakthrough in AF catheter ablation was made by Michel Haîssaguerre and his team. They observed that a vast majority of AF was initiated by triggers from a focal source in the pulmonary veins (PVs), and ablation of the focal sources terminated AF.8 In 2000, Carlo Pappone and colleagues demonstrated the safety and effectiveness of circumferential radiofrequency (RF) ablation of the PV ostia to terminate paroxysmal or permanent AF. This approach came to be known as wide area circumferential ablation (WACA).8
New Developments in EP
Our goal is to advance the management and treatment of cardiac arrhythmias. We focus on providing a bridge between basic electrical, chemical, and bioengineering advances, and adopting these and other innovative solutions in preclinical models. In addition to our internal resources, we have fostered very fruitful collaborations with scientists at Rice University and Texas A&M University. These collaborations have led to a number of advances which are summarized here.
Promising data in mouse model to restore myocardial conduction with carbon nanotube fibers
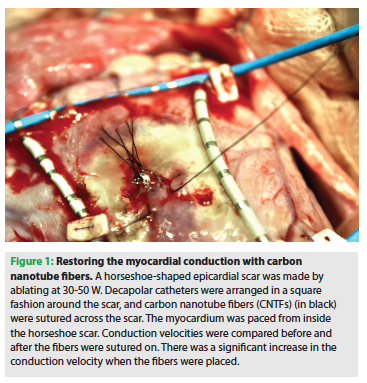 Myocardial ischemia reduces myocardial conduction velocity, which causes conduction block and ventricular tachycardia. Our team previously showed that carbon nanotube fibers (CNTFs), developed at Professor Matteo Pasquali’s lab at Rice University, have the unique properties of electrical conductivity along with flexibility and fatigue resistance. When sewn across epicardial scar in a surgical sheep model, CNTFs restore physiologic transmyocardial conduction velocity through myocardial scar (Figure 1). In recent experiments performed at the Texas Heart Institute and at the University of Sassari, Mark McCauley (currently at the University of Illinois at Chicago) and our colleague Professor Lucia Gemma Delogu studied the toxicity profile of CNTF in living systems. To determine the biocompatibility and non-toxicity of CNTF in organic systems, CNTF interaction with human whole blood was evaluated (ex vivo) — including in mice — for up to three months. These ex vivo and in vivo studies showed that CNTF did not cause significant inflammatory tissue response, foreign body reaction, or excessive growth of fibrous tissue. Thus, CNTF was demonstrated to be a unique conductive and biocompatible material to restore electrical conduction in diseased myocardium; it may provide a long-term treatment solution for diseased and electrically excitable tissues. In 2015, Drs. Pasquali and Medhi Razavi were recognized for their work with a Collaborative Sciences Award from the American Heart Association (AHA).
Myocardial ischemia reduces myocardial conduction velocity, which causes conduction block and ventricular tachycardia. Our team previously showed that carbon nanotube fibers (CNTFs), developed at Professor Matteo Pasquali’s lab at Rice University, have the unique properties of electrical conductivity along with flexibility and fatigue resistance. When sewn across epicardial scar in a surgical sheep model, CNTFs restore physiologic transmyocardial conduction velocity through myocardial scar (Figure 1). In recent experiments performed at the Texas Heart Institute and at the University of Sassari, Mark McCauley (currently at the University of Illinois at Chicago) and our colleague Professor Lucia Gemma Delogu studied the toxicity profile of CNTF in living systems. To determine the biocompatibility and non-toxicity of CNTF in organic systems, CNTF interaction with human whole blood was evaluated (ex vivo) — including in mice — for up to three months. These ex vivo and in vivo studies showed that CNTF did not cause significant inflammatory tissue response, foreign body reaction, or excessive growth of fibrous tissue. Thus, CNTF was demonstrated to be a unique conductive and biocompatible material to restore electrical conduction in diseased myocardium; it may provide a long-term treatment solution for diseased and electrically excitable tissues. In 2015, Drs. Pasquali and Medhi Razavi were recognized for their work with a Collaborative Sciences Award from the American Heart Association (AHA).Possible role of bioimpedance measurements to improve the safety of percutaneous pericardial access
Access to the pericardial space is necessary for epicardial mapping and ablation or for LARIAT (SentreHEART, Inc.) procedures.9,10 Percutaneous pericardial access is obtained through a subxiphoid pericardial puncture and by advancing the needle into the pericardial space under fluoroscopy or ultrasound guidance.11 However, the subxiphoid approach can be challenging for physicians, and is associated with complications such as ventricular puncture, pleuropericardial fistula, coronary artery/vein laceration, and visceral injuries.11 In this study, our aim was to develop a device that allowed physicians better navigation into the pericardial space with reduced risks. We explored the use of bioimpedance as a tool to provide real-time navigation. Our preliminary studies in Suffolk-cross sheep (n=3) were aimed at collecting bioimpedance data outside of the pericardium, inside the pericardial space, and inside the right ventricle. The results from these studies had potential, and showed that bioimpedance in the pericardial space was significantly different from the anterior mediastinum and right ventricle. Having secured these promising results, our group aims to develop a device that will allow for real-time navigation into the pericardial space.
Deformation of the esophagus to mitigate risk of atrio-esophageal fistula
Radiofrequency ablation of atrial fibrillation may result in a rare but life-threatening complication, atrio-esophageal fistula (AEF).12 Several approaches are used to prevent esophageal injury during RF ablation. The essential step is to determine the location of the esophagus prior to RF ablation in order to avoid radiofrequency delivery within 1 cm of the esophagus.13 Previous studies have shown that mechanical deflection of the esophagus during catheter RF ablation could result in avoidance of accidental esophageal thermal lesions.14,15
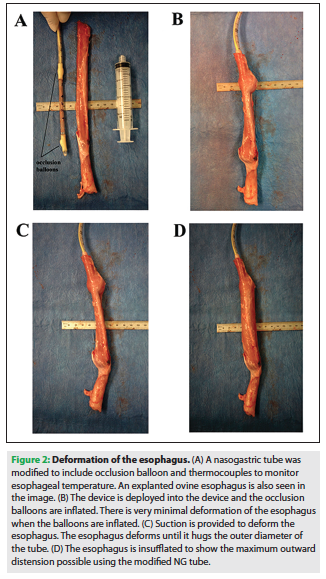 In our study, we explored the use of an original device to deform the esophagus and continually monitor luminal temperature to prevent atrio-esophageal fistula complications. A modified nasogastric tube (18 Fr) (Figure 2) was placed in the esophagus of porcine and ovine cadavers to deform the esophagus and monitor the internal temperature of the esophagus. The extent of deformation of the esophagus was calculated in situ and in excised specimens. The native size of the esophagus was found to be 18.5 ± 4.1 mm. Placement of the device and applying suction through the openings on the tube reduced the width to 13.1 ± 2.3 mm. Deformation of the esophagus was easily achieved by use of the modified nasogastric tube. This finding has paved the way to the possibility of further developing simple devices to protect the esophagus during RF ablation.
In our study, we explored the use of an original device to deform the esophagus and continually monitor luminal temperature to prevent atrio-esophageal fistula complications. A modified nasogastric tube (18 Fr) (Figure 2) was placed in the esophagus of porcine and ovine cadavers to deform the esophagus and monitor the internal temperature of the esophagus. The extent of deformation of the esophagus was calculated in situ and in excised specimens. The native size of the esophagus was found to be 18.5 ± 4.1 mm. Placement of the device and applying suction through the openings on the tube reduced the width to 13.1 ± 2.3 mm. Deformation of the esophagus was easily achieved by use of the modified nasogastric tube. This finding has paved the way to the possibility of further developing simple devices to protect the esophagus during RF ablation.A wireless, battery-less pacemaker
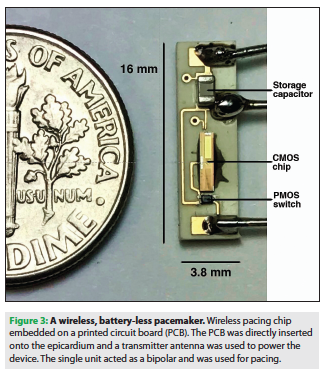 Novel wireless pacing devices have allowed physicians to reduce the complications associated with traditional pacemaker leads16; however, wireless pacing mechanisms are still dependent on an incorporated battery, which increases the overall bulk and size of the device. This size restriction may lead to limited placement location and increased risk of dislodgement and embolism.16 We are working with several professors — primarily Dr. Aydin Babakhani (who developed the technology) and Dr. Behnaam Aazhang from Rice University Electrical and Computer Engineering, as well as Dr. Farshad Raissi at UCSD — to develop a wireless, battery-less pacemaker system that harvests energy from RF radiation transmitted by an external battery pack.17 Recently, we tested the feasibility of a wirelessly powered microchip that can be implanted directly into the heart to capture ventricular myocardium. A microchip (4 x 1 mm), which was placed on a 16 x 3.8 mm printed circuit board, was utilized to provide pacing to an ovine model (Figure 3).
Novel wireless pacing devices have allowed physicians to reduce the complications associated with traditional pacemaker leads16; however, wireless pacing mechanisms are still dependent on an incorporated battery, which increases the overall bulk and size of the device. This size restriction may lead to limited placement location and increased risk of dislodgement and embolism.16 We are working with several professors — primarily Dr. Aydin Babakhani (who developed the technology) and Dr. Behnaam Aazhang from Rice University Electrical and Computer Engineering, as well as Dr. Farshad Raissi at UCSD — to develop a wireless, battery-less pacemaker system that harvests energy from RF radiation transmitted by an external battery pack.17 Recently, we tested the feasibility of a wirelessly powered microchip that can be implanted directly into the heart to capture ventricular myocardium. A microchip (4 x 1 mm), which was placed on a 16 x 3.8 mm printed circuit board, was utilized to provide pacing to an ovine model (Figure 3).  The microchip had an on-chip receiving antenna to receive incoming radiofrequency (GHz), and converted the electromagnetic signal from AC to DC power. The generated power was then stored briefly in a capacitor and outputted using a digital switch. The standard pacing leads were sutured to the epicardial surface to pace the heart. A decapolar catheter was sutured on the ventricle to characterize the electrophysiology of the heart, and the LABSYSTEM PRO EP Recording System (Boston Scientific) was used to collect data from this catheter. The result of this study showed that with an output of 1.3V and pulse-width of 2 ms, this innovative new pacemaker — without the need for an on-board battery — was capable of epicardial capture at various cycle lengths in an ovine model. These findings support the possibility of developing a pacemaker with improved overall function that poses far less complications.
The microchip had an on-chip receiving antenna to receive incoming radiofrequency (GHz), and converted the electromagnetic signal from AC to DC power. The generated power was then stored briefly in a capacitor and outputted using a digital switch. The standard pacing leads were sutured to the epicardial surface to pace the heart. A decapolar catheter was sutured on the ventricle to characterize the electrophysiology of the heart, and the LABSYSTEM PRO EP Recording System (Boston Scientific) was used to collect data from this catheter. The result of this study showed that with an output of 1.3V and pulse-width of 2 ms, this innovative new pacemaker — without the need for an on-board battery — was capable of epicardial capture at various cycle lengths in an ovine model. These findings support the possibility of developing a pacemaker with improved overall function that poses far less complications. Disclosures: The authors have no conflicts of interest to report regarding the content herein. Outside the submitted work, the following was disclosed. Mr. Ganapathy reports personal fees from Saranas, a patent pending for the pericardial wire device, and a patent pending for the wireless pacemaker device. Dr. Greet reports intellectual property rights for both bioimpedance measurements in pericardial space and the wireless pacemaker. Dr. Burkland reports patents pending for the pericordial impedance based access and navigation system and multipoint wireless pacemaker. Dr. Mehdi Razavi reports intellectual property rights for nanofibers, esophageal, and the wireless pacemaker.
References
- Waller AD. A Demonstration on Man of Electromotive Changes accompanying the Heart’s Beat. J Physiol. 1887;8(5):229-234.
- Fisch C. Centennial of the string galvanometer and the electrocardiogram. J Am Coll Cardiol. 2000;36(6):1737-1745.
- Rivera-Ruiz M, Cajavilca C, Varon J. Einthoven’s String Galvanometer: The First Electrocardiograph. Tex Heart Inst J. 2008;35(2):174-178.
- Braunwald E. The Simon Dack lecture. Cardiology: the past, the present, and the future. J Am Coll Cardiol. 2003;42:2031-2041.
- Aquilina O. A brief history of cardiac pacing. Images Paediatr Cardiol. 2006;8(2):17-81.
- Van der Wall EE. Milestones in cardiovascular medicine: 10 or more? Neth Heart J. 2013;21(12):527-529.
- Van Welsenes GH, Borleffs CJW, van Rees JB, et al. Improvements in 25 Years of Implantable Cardioverter Defibrillator Therapy. Neth Heart J. 2011;19(1):24-30.
- Safavi-Naeini P, Razavi M, Massumi A, et al. Review: Focal Impulse and Rotor Modulation (FIRM) Ablation. EP Lab Digest. 2014;14(6):32,35.
- Della Bella P, Brugada J, Zeppenfeld K, et al. Epicardial ablation for ventricular tachycardia: a European multicenter study. Circ Arrhythm Electrophysiol. 2011;4:653-659.
- Sievert H, Rasekh A, Bartus K, et al. Left atrial appendage ligation in nonvalvular atrial fibrillation patients at high risk for embolic events with ineligibility for oral anticoagulation. Initial report of clinical outcomes. JACC Clin Electrophysiol. 2015;1(6):465-474.
- Gunda S, Reddy M, Pillarisetti J, et al. Differences in Complication Rates Between Large Bore Needle and a Long Micropuncture Needle During Epicardial Access. Circ Arrhythm Electrophysiol. 2015;8:890-895.
- Chavez P, Messerli FH, Casso Dominguez A, et al. Atrioesophageal fistula following ablation procedures for atrial fibrillation: systematic review of case reports. Open Heart. 2015;2:1-9.
- Gilcrease GW, Stein JB. A delayed case of fatal atrioesophageal fistula following radiofrequency ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2010;21:708-711.
- Mateos JC, Mateos E, Peña TG, et al. Simplified method for esophagus protection during radiofrequency catheter ablation of atrial fibrillation--prospective study of 704 cases. Rev Bras Cir Cardiovasc. 2015;30(2):139-147.
- Shuraih M, Frederick M, Shivkumar K, Buch E. Strategies to Prevent Esophageal Injury During Catheter Ablation of Atrial Fibrillation. The Journal of Innovations in Cardiac Rhythm Management. 2012;3:719-726.
- Bernard ML. Pacing Without Wires: Leadless Cardiac Pacing. Ochsner J. 2016;16(3):238-242.
- Texas team debuts battery-less pacemaker. Rice University News & Media. Published June 5, 2017. Available online at https://news.rice.edu/2017/06/05/texas-team-debuts-battery-less-pacemaker/. Accessed July 12, 2017.

Current Issue
April 2025
Volume 24
Issue 4
Stay in the know.
EP Lab Digest Newsletter
