

Left Atrial Thrombus Aspiration Guided by ICE During Catheter Ablation for Atrial Fibrillation Utilizing Cerebral Protection Devices
Case Report
A 76-year-old female presented to the EP clinic with a 3-year history of paroxysmal atrial fibrillation. She had tried multiple antiarrhythmics including dronedarone and sotalol, but had recurrence of her atrial fibrillation. She had also undergone multiple direct current cardioversions, only to have breakthrough episodes of atrial fibrillation. The patient is very symptomatic, citing fatigue, lack of energy, and palpitations as her primary symptoms.
At the time of evaluation, she was deemed to be in persistent atrial fibrillation and was consequently scheduled for radiofrequency ablation. Prior to the procedure, the patient underwent a CT scan of the chest to evaluate the pulmonary vein anatomy. The patient was also chronically anticoagulated with warfarin, and her international normalized ratio (INR) on the day of the procedure was 2.43.
She was then brought to the EP lab where the procedure would be performed under general anesthesia. Upon arrival to the EP lab, she was in atrial fibrillation with controlled ventricular response. Standard venous access was obtained using three 8 French (Fr) sheaths inserted into the right common femoral vein using ultrasound guidance. A 9 Fr sheath was inserted into the left common femoral vein as well as a 7 Fr sheath into the right internal jugular vein. A preprocedural transesophageal echocardiogram (TEE) confirmed the absence of intraatrial thrombus. The anatomy from the TEE as well as a 64-slice CAT scan was integrated with electroanatomical mapping anatomy obtained from the EnSite Velocity System (St. Jude Medical). Once vascular access was obtained, a duodecapolar catheter was inserted through the right internal jugular vein into the coronary sinus with the proximal poles in the high right atrium. Next, a right ventricular quadripolar catheter was inserted into the right ventricle and an intracardiac echo (ICE) catheter was placed via the left femoral vein into the RA.
Next, transseptal puncture was done using the ACross Transseptal Access System (St. Jude Medical) and SafeSept® needle (Pressure Products) under ICE and hemodynamic guidance. The spiral catheter was then advanced into the transseptal sheath into the left atrium. Electroanatomical mapping of the left atrium was then completed. Due to difficult anatomy, we were unable to engage the left inferior pulmonary vein and had to exchange the spiral catheter with the ablating catheter to help obtain the rest of the anatomical mapping. During exchange and removal of the spiral catheter, aspiration was done and thrombus was discovered in the sheath. The patient was then given 6500 U of heparin, and an ACT of 400 seconds was maintained throughout the rest of the procedure. Multiple aspirations were done for the clotted sheath and an extra 2000 units of heparin were injected through the sheath to ensure absence of any thrombus.
As a result of the thrombus being found, the patient was then awoken from anesthesia and extubated, and a full neurological examination was undertaken. A full motor function, sensory function, and cranial nerve evaluation was obtained with no observable deficits noted. The patient was then re-intubated and sedated under general anesthesia, and the procedure was resumed once again. At this time, a second transseptal puncture was pursued under ICE guidance, and we placed an ablating catheter in this 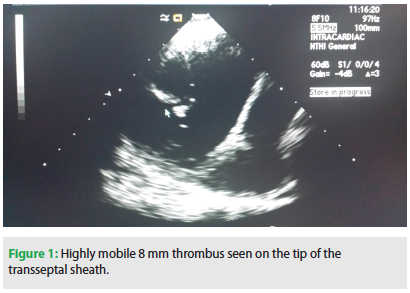 second sheath.
second sheath.
After advancing the spiral catheter inside the first transseptal sheath, a mobile thrombus was visualized under ICE in the left atrium (Figure 1). Upon further review of these images, it was found that the thrombus was attached to the distal end of the sheath where the spiral catheter was protruding.
Prior to making an attempt to evacuate the thrombus from the sheath, two temporary filters were placed in the carotids bilaterally to help protect the patient’s neurological status in case inadvertent dislodgement of thrombus occurred during aspiration; this was done in a timely way with our interventional cardiologist. Specifically, a Cordis filter basket was placed in the right carotid and an Emboshield NAV6 Embolic Protection System (Abbott Vascular) in the left common carotid artery was deployed. This was achieved by placing two arterial lines into both groins under SonoSite access above the bifurcation. Once this was accomplished and the filters were in place, we proceeded to aspirate about 70ml of blood from the left atrium under ICE  guidance. During the aspiration, we were able to retrieve the mobile thrombus with direct visualization of the thrombus that came out of the syringe. The thrombogenic sheath was then removed and a fresh sheath was inserted using a third transseptal puncture. The two carotid umbrellas were then removed (Figures 3 and 4), and there were no thrombi seen in the umbrellas. Bilateral cerebral angiograms were performed showing no evidence of embolization. Multiple flushes with heparin and aspirations were made during the sheath exchanges, without evidence of thrombus recurrence throughout the rest of the procedure.
guidance. During the aspiration, we were able to retrieve the mobile thrombus with direct visualization of the thrombus that came out of the syringe. The thrombogenic sheath was then removed and a fresh sheath was inserted using a third transseptal puncture. The two carotid umbrellas were then removed (Figures 3 and 4), and there were no thrombi seen in the umbrellas. Bilateral cerebral angiograms were performed showing no evidence of embolization. Multiple flushes with heparin and aspirations were made during the sheath exchanges, without evidence of thrombus recurrence throughout the rest of the procedure.
Upon resumption of the ablation process, we were able to achieve pulmonary vein isolation and left atrial roof line, followed by mitral annular line. Bidirectional block was achieved for the lines. Isuprel was then given (up to 20 mcg), increasing the heart rate to 120 bpm without evidence of atrial fibrillation. There were occasional PACs originating from the coronary sinus os. Consequently, a few lesions were created to eliminate coronary sinus os triggers.
The patient was then awaked from general anesthesia and extubated. A full motor, sensory, and cranial nerve assessment was again obtained, with no neurological deficits noted clinically. Long-term follow-up of the patient showed freedom of atrial fibrillation 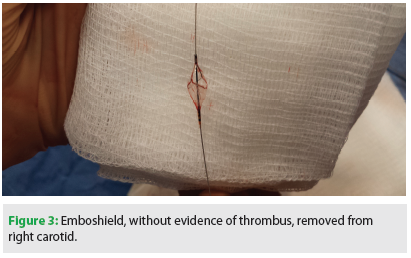 and CVA.
and CVA.
Discussion
The occurrence of left atrial thrombus formation on the transseptal sheath or mapping catheters, detected by ICE, has been reported in 10.3% of patients undergoing radiofrequency ablation for AF despite anticoagulation with heparin to ACT >250 seconds.1 To date, there have not been a lot of prospective, randomized studies done regarding the optimal approach to reduce the thromboembolic risk in the periablation period.2 Therefore, data is scarce for optimal strategies to help prevent thrombus formation.
The few studies that have been done thus far have shown that higher concentrations of heparin with a target ACT >300 seconds, starting heparin before the transseptal puncture, and performing the ablation on patients with therapeutic INR do reduce the risk 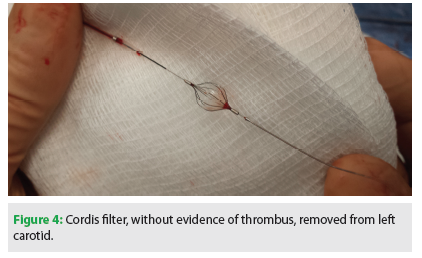 of thrombus formation.3-5 These strategies have become the standard of practice in efforts to help reduce the risk of thrombus formation.
of thrombus formation.3-5 These strategies have become the standard of practice in efforts to help reduce the risk of thrombus formation.
Our case demonstrates the importance of utilizing heparin prior to transseptal puncture to avoid sheath thrombus formation. It also emphasizes the importance of disposition of the sheath once thrombus is seen during aspiration, as rigorous flushing and heparinization are inadequate to ensure complete removal of the thrombus from the sheath. In addition, this case illustrates that taking the extra steps to insert protection filters is feasible prior to aspiration of the thrombus. Given the high mobility of the thrombus, it could have been dislodged if we had simply dragged it to the right atrium. It is also important to note that ICE has the advantage of allowing early detection of intracardiac thrombus, thus allowing early intervention for thrombus removal.6
Safety Tips
- Aspirate long sheaths before catheter exchanges.
- Administer heparin before transseptal punctures.
- Note disposition of the sheath once thrombus is seen during aspiration; rigorous flushing and heparinization are inadequate to ensure complete removal of the thrombus from the sheath.
- Maintain higher ACT (>400) once thrombus is seen.
- Carotid devices may be implemented prior to aspiration for fear of cerebral embolization.
- Ensure there are no neurological deficits by awakening the patient prior to completion of the ablation; this may be important, as early use of thrombolytic may be needed should neurological deficit occur.
- Intracardiac echo is very helpful for early detection and treatment of intracardiac thrombi.
- Utilize continuous heparinized saline flow for long sheaths during procedure.
Conclusion
Left atrial thrombi are commonly seen in EP procedures; however, limited literature on management is available. This case study shows how early detection and retrieval of a large mobile thrombus by catheter aspiration, with the help of intracardiac echo and cerebral protection devices, allowed for a favorable outcome.
Disclosures: The authors have no conflicts of interest to report regarding the content herein.
References
- Ren JF, Marchlinski FE, Callans DJ. Left atrial thrombus associated with ablation for atrial fibrillation: identification with intracardiac echocardiography. J Am Coll Cardiol. 2004;43:1861-1867.
- Natale A, Raviele A, Arentz T, et al. Venice Chart international consensus document on atrial fibrillation ablation. J Cardiovasc Electrophysiol. 2007;18:560-580.
- Ren JF, Marchlinski FE, Callans DJ, et al. Increased intensity of anticoagulation may reduce risk of thrombus during atrial fibrillation ablation procedures in patients with spontaneous echo contrast. J Cardiovasc Electrophysiol. 2005;16:474-477.
- Bruce CJ, Friedman PA, Narayan O, Munger TM, Hammill SC, Packer DL, Asirvatham SJ. Early heparinization decreases the incidence of left atrial thrombi detected by intracardiac echocardiography during radiofrequency ablation for atrial fibrillation. J Interv Card Electrophysiol. 2008;22:211-219.
- Wazni OM, Beheiry S, Fahmy T, et al. Atrial fibrillation ablation in patients with therapeutic international normalized ratio: comparison of strategies of anticoagulation management in the periprocedural period. Circulation. 2007;116:2531-2534.
- Keane D, Mansour M, Singh J. Detection by intracardiac echocardiography of early formation of left atrial thrombus during pulmonary vein isolation. Europace. 2004;6:109-110.

