

Innovations in Electroanatomic Mapping: Ultra-High Density Mapping
The success of electrophysiologic studies and ablation rests on the careful analysis of electrograms in sinus rhythm and arrhythmia as well as the performance and assessment of dynamic pacing maneuvers. However, the effectiveness of catheter ablation  often relies heavily on the accuracy, resolution, and fidelity of electroanatomic mapping as well. Over the years, the development and evolution of electroanatomic mapping systems has greatly facilitated the efficacy and safety of catheter ablation procedures. Catheter ablation has enhanced the management of common arrhythmias such as atrial fibrillation, and drastically altered treatment strategies for ventricular tachyarrhythmias. Early mapping relied heavily on point-to-point annotation with bipolar mapping catheters. Advances in mapping have included improved accuracy of electroanatomic shells and localization, the use of noncontact mapping with multielectrode arrays, and the advent of multipolar catheters to enhance both surface collection in sinus rhythm as well as mapping during arrhythmia. Despite the development of electroanatomic mapping systems, the effectiveness and utilization of catheter ablation is often limited by operator skill, dependence on map accuracy, and the complexity of electroanatomic map creation.
often relies heavily on the accuracy, resolution, and fidelity of electroanatomic mapping as well. Over the years, the development and evolution of electroanatomic mapping systems has greatly facilitated the efficacy and safety of catheter ablation procedures. Catheter ablation has enhanced the management of common arrhythmias such as atrial fibrillation, and drastically altered treatment strategies for ventricular tachyarrhythmias. Early mapping relied heavily on point-to-point annotation with bipolar mapping catheters. Advances in mapping have included improved accuracy of electroanatomic shells and localization, the use of noncontact mapping with multielectrode arrays, and the advent of multipolar catheters to enhance both surface collection in sinus rhythm as well as mapping during arrhythmia. Despite the development of electroanatomic mapping systems, the effectiveness and utilization of catheter ablation is often limited by operator skill, dependence on map accuracy, and the complexity of electroanatomic map creation.
Fortunately, we are in the midst of a period of rapid technologic advancement in electroanatomic mapping and catheter ablation. New techniques to dramatically reduce fluoroscopic exposure,1 allow panoramic mapping of rotors in atrial fibrillation,2 and contact-force sensing3 are all recent and notable advances in the field. However, technologic advances in rapid, automated electrogram acquisition also offer a promising pathway for improved efficiency, efficacy, and safety in the EP lab.
About the Technology
The Rhythmia™ Mapping System (Boston Scientific) is a new electroanatomic mapping system that can provide very high-resolution information about activation sequence and myocardial scar in an automated fashion. More detailed and rapid activation mapping has great potential to improve the efficacy and safety of catheter ablation, and to better delineate the mechanisms of common arrhythmias. 
The Rhythmia system utilizes both magnetic-based (resolution ≤1 mm) and impedance-based (resolution ≤2 mm) localization. Accordingly, the system uses two location references: a magnetic location reference back patch and a stationary system electrode reference (usually the coronary sinus catheter). The system is optimally designed to work with the IntellaMap Orion™ High Resolution Mapping Catheter (Boston Scientific). The IntellaMap Orion Catheter has 64 imprinted electrodes with 2.5 mm inter-electrode spacing on 8 nitinol splines. The catheter is 8.5 Fr with bi-directional deflection and a variable mini-basket diameter (3-22 mm) that can be adjusted based upon the anatomic needs (Figure 1). The use of a magnetically-tracked catheter is coupled with the impedance mapping, such that the system tracks impedance measurements at each location during creation and validation of the magnetic-based map. Both beat-to-beat mapping and continuous mapping can be performed with the system. In contrast to traditional beat-to-beat mapping, rapid and automated mapping is mediated through continuous mapping via user-defined beat acceptance criteria. These criteria are established after induction of an arrhythmia and incorporate multiple variables, including cycle length, respiratory phase, propagation reference (most frequently for atrial mapping), ECG morphology (for ventricular mapping), electrogram stability, catheter motion (used to avoid data when the catheter is moving fast), and ventricular signal overlap (Figure 2). These criteria also allow the system to discern a particular tachycardia or morphology in the presence of multiple arrhythmias or complex ectopy.
Early Experience
Early preclinical work in animal models suggests that the system can acquire a very high number of points in a very limited period of time (median 3589 electrograms over a median of 7.3 minutes of mapping time) with acceptable accuracy (median 2.7 mm resolution) and efficacy. In a canine atrial lesion model, investigators achieved 100% block across all targeted linear gap lesions (n=10).4 Additional animal work has demonstrated that high-density mapping allows fast, simple, and very detailed assessment of sinus node activation, allowing quick delineation of sinus break-out and earliest activation.5 Perhaps the greatest promise and utility of high-density electroanatomic mapping lies in cases with complex myocardial substrate and tachycardia propagation, such as those encountered in ablation of ventricular tachycardia. While the use of multielectrode catheters to facilitate mapping in the ventricles is certainly not a new concept,6 advances in high-density mapping again appear to yield incremental advantage. In 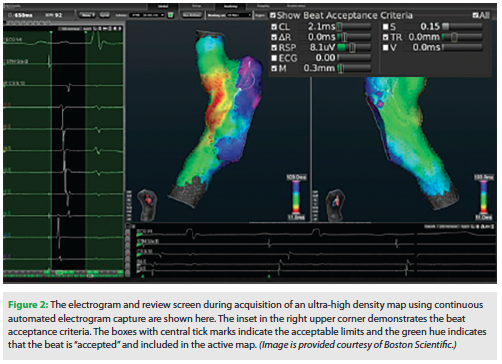 canine chronic infarct models (n=5), the use of high-density mapping was able to characterize 7754 ± 1960 electrograms per animal with a mean resolution of 2.8 ± 0.6 mm.7 These maps included the identification of more than 200 isolated low amplitude late potentials per animal/ventricle. Finally, unipolar voltage correlated well with scar as defined by cardiac MRI.7 Additional work from other investigators have shown similar findings with mini-basket catheter mapping of VT in animal models, including poorly tolerated VT.8
canine chronic infarct models (n=5), the use of high-density mapping was able to characterize 7754 ± 1960 electrograms per animal with a mean resolution of 2.8 ± 0.6 mm.7 These maps included the identification of more than 200 isolated low amplitude late potentials per animal/ventricle. Finally, unipolar voltage correlated well with scar as defined by cardiac MRI.7 Additional work from other investigators have shown similar findings with mini-basket catheter mapping of VT in animal models, including poorly tolerated VT.8
While the published data on ultra-high density mapping with the Rhythmia system is largely confined to preclinical work, early experience in the clinical arena is beginning to accrue and emerging data will be presented at Heart Rhythm 2015. Early work in our laboratory has confirmed the utility of the system in creating high-resolution electroanatomic maps in minutes. The detail associated with high-density mapping allows excellent visualization of tachycardia circuits, including common arrhythmias that are often not well-visualized with conventional mapping systems. For example, Video 1 and Video 2 demonstrate a propagation map of sinus rhythm and typical atrioventricular nodal reentrant tachycardia with anterograde conduction down the slow pathway and retrograde conduction up the fast pathway. The propagation map of AVNRT includes over 4000 electrograms collected in a little over 3 minutes.
Summary
Time will tell if rapid and automated acquisition of high-density electroanatomic mapping will lead to improved outcomes in the EP laboratory. These outcomes might include decreased fluoroscopy time, procedural time, total radiofrequency ablation delivery, arrhythmia recurrence, and improved freedom from drug therapy. Future studies should focus on direct, randomized head-to-head comparisons of mapping techniques. Finally, ultra-high density high-resolution mapping should help facilitate the understanding of the underlying anatomic or mechanistic basis of arrhythmia by facilitating the visualization of arrhythmia circuits.
Disclosures: Dr. Piccini receives research funding from ARCA biopharma, Boston Scientific, Gilead, Janssen Pharmaceuticals, ResMed and St. Jude Medical. He serves as a consultant to Johnson & Johnson, Laguna Pharmaceuticals, Medtronic, and Spectranetics.
References
- Sommer P. Nonfluoroscopic catheter tracking: toy or tool? Pacing Clin Electrophysiol. 2015 Feb 16. [Epub ahead of print]
- Narayan SM, Patel J, Mulpuru S, Krummen DE. Focal impulse and rotor modulation ablation of sustaining rotors abruptly terminates persistent atrial fibrillation to sinus rhythm with elimination on follow-up: a video case study. Heart Rhythm. 2012;9:1436-1439.
- Natale A, Reddy VY, Monir G, et al. Paroxysmal af catheter ablation with a contact force sensing catheter: results of the prospective, multicenter SMART-AF trial. J Am Coll Cardiol. 2014;64:647-656.
- Nakagawa H, Ikeda A, Sharma T, Lazzara R, Jackman WM. Rapid high resolution electroanatomical mapping: evaluation of a new system in a canine atrial linear lesion model. Circ Arrhythm Electrophysiol. 2012;5:417-424.
- Bollmann A, Hilbert S, John S, Kosiuk J, Hindricks G. Insights from preclinical ultra high-density electroanatomical sinus node mapping. Europace. 2015;17:489-494.
- Eldar M, Fitzpatrick AP, Ohad D, et al. Percutaneous multielectrode endocardial mapping during ventricular tachycardia in the swine model. Circulation. 1996;94:1125-1130.
- Thajudeen A, Jackman WM, Stewart B, et al. Correlation of scar in cardiac MRI and high-resolution contact mapping of left ventricle in a chronic infarct model. Pacing Clin Electrophysiol. 2015 Feb 6. [Epub ahead of print]
- Tanaka Y, Genet M, Chuan Lee L, Martin AJ, Sievers R, Gerstenfeld EP. Utility of high-resolution electroanatomic mapping of the left ventricle using a multispline basket catheter in a swine model of chronic myocardial infarction. Heart Rhythm. 2015;12:144-154.

