

Initial Human Experience of a Novel Steerable Sheath for AF Ablation With Circumferential PV Isolation
Pulmonary vein ablation, also called pulmonary vein antrum isolation or PVAI, is the accepted treatment for atrial fibrillation (AF) and offers a potential curative strategy for patients with AF. Data continues to show that AF ablation is superior to the currently available antiarrhythmic medications in maintaining sinus rhythm.1
Despite superior results over pharmaceutical regimens, success rates vary with current ablation techniques and technologies. AF ablation procedures often extend beyond three hours and require various mapping strategies, multiple lesions, and at times, repeat procedures. While success rates have been promising, the reoccurrence of AF remains relatively high at one year.2
It is widely accepted that stable access to the left atrial (LA) targets and sufficient contact force between the ablation catheter tip and the endocardial surface are essential for the creation of successful lesions.3 Long sheaths are commonly used to enhance ablation catheter steerability and improve tip-to-tissue contact force during PV isolation. Traditionally, fixed curve transseptal sheaths of various shapes and sizes have been used. However, recently developed steerable sheaths have further improved left atrial access, maneuverability, and tissue contact.
Steerable sheaths allow the operator to alter the sheath shape and improve manipulation of the catheter in the left atrium. The sheaths increase the stability of the catheter during ablation and allow easier access to difficult regions such as the right inferior pulmonary vein. Existing steerable sheath designs use pull-wires to generate tip deflection, which can cause abrupt catheter movements as a result of torque buildup. This whipping effect is frustrating and can cause physicians to lose a desired catheter position, which lengthens the procedure time. The Vado® Steerable Sheath with truVector™ Technology (Kalila Medical) has an innovative coaxial design that does not require pull-wires and improves sheath stability in difficult to access LA regions (Figure 1).  We conducted a First-in-Human study to compare the Vado Sheath to currently available sheaths in our lab.
We conducted a First-in-Human study to compare the Vado Sheath to currently available sheaths in our lab.
First-In-Human Case Description
The first-in-human use of the novel Vado Steerable Sheath took place in October 2014 at Christchurch Hospital with three operators. We treated eight patients with recurring paroxysmal or persistent atrial fibrillation (six males and two females, ranging from 42-69 years).
The Vado Sheath was different from previous sheaths used at our institution, because the steerable design did not require pull-wires to create tip deflection. The 8.8F ID sheath design employs truVector Technology with a coaxial lumen, an inner shaft and outer shaft, bonded together at the distal tip and attached to two reference locations at the proximal end within the handle. Similar to existing steerable sheaths, tip deflection is achieved by rotating a knob on the sheath handle. In contrast to pull-wire designs, the Vado Sheath handle mechanism creates proximal tension on the inner shaft resulting in unilateral tip deflection since the two shafts are joined distally. This action pulls on the inner shaft, which causes tip deflection up to 270˚ (Figure 2). By eliminating 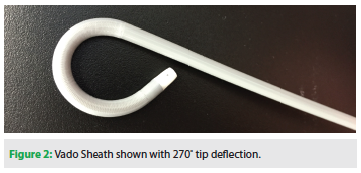 pull-wires, the Vado Sheath provides stable tip deflection during catheter rotations and improves torque transfer to the distal catheter.
pull-wires, the Vado Sheath provides stable tip deflection during catheter rotations and improves torque transfer to the distal catheter.
The Vado Sheath was used to cross the atrial septum using either an 89 cm Brockenbrough (Medtronic, Inc.) or an 89 cm HeartSpan® Transseptal Needle (Biosense Webster, Inc., a Johnson & Johnson company). Patients were ablated with primarily D- or F-type, irrigated tip, NaviStar ThermoCool catheters or 20 mm Lasso catheters. The Carto® Mapping System (Biosense Webster, Inc., a Johnson & Johnson company) was used for six patients, while the remaining two patients were treated with the Arctic Front cryoablation system (Medtronic, Inc.). Patients were on therapeutic anticoagulation, with international normalized ratio (INR) maintained between 2.0 and 3.0 with warfarin. Antiarrhythmic drugs were discontinued five days prior to the procedure. All procedures were performed under local anesthesia with conscious sedation of midazolam and fentanyl. Heparin was administered to maintain an activated clotting time of >300 s through the procedure. Lesions were created in all patients, and only one patient required cardioversion.
Clinical Results
All eight patients were successfully ablated with the assistance of the Vado Sheath, including two patients who were repeat ablations requiring only superior vein isolation. Procedure times ranged from 170-260 minutes; fluoroscopy time, radiation dose, and 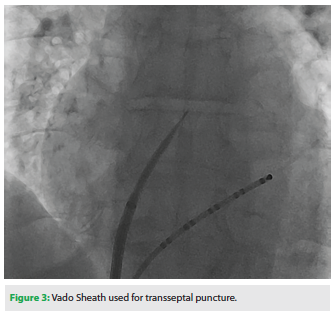 burn times were also within normal ranges.
burn times were also within normal ranges.
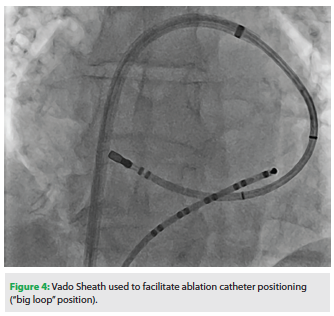
We believe the Vado Sheath significantly improved ablation catheter manipulation and our ability to target veins in the left atrium. Catheter stability was also improved when using the Vado Sheath as compared to the ablation catheter alone. The sheath had excellent visibility under fluoroscopy due to an enhanced dilator radiopacity (Figure 3). Engagement of the fossa ovalis and transseptal puncture using the Vado Sheath was easy to perform and was facilitated by the variable curve. Ablation and Lasso catheters were easily positioned in the left atrium (Figure 4). We found excellent torque transmission when using the Vado Sheath, and no abrupt catheter movements were observed.
No procedural complications were reported during the study. Post-procedural adverse events occurred in three patients unrelated to the Vado Sheath. One patient suffered gastrointestinal distress, one patient experienced a migraine, and one patient was hospitalized with mild pneumonia. All events resolved in 1.5 days.
Conclusions 
Stable and controlled catheter manipulation in the left atrium is crucial to ensure good tip-to-tissue catheter contact and create successful ablation lesions. The Vado Sheath, a novel coaxial steerable sheath design without pull-wires, improved our ability to target and isolate veins in patients with paroxysmal and persistent AF.
The Vado Sheath offers a simple solution to improve patient outcomes for AF ablation by removing the limitations of fixed curve sheaths, which can have poor maneuverability, and existing pull-wire steerable sheaths, which are prone to abrupt movements.
Further evaluations are ongoing in Europe and the United States. The Vado Steerable Sheath is FDA cleared for sale in the U.S., and CE mark approved for distribution in Europe.
Disclosures: Dr. Crozier reports grants from Kalila Medical. Dr. Melton reports grants from Kalila Medical, and outside the submitted work, reports personal fees from Medtronic and Boston Scientific as a clinical advisory board member. Dr. Daly has no conflicts of interest to report regarding the content herein. Ms. Cruickshank reports grants from Kalila Medical.
References
- Cleland JG, Coletta AP, Buga L, Ahmed D, Clark AL. Clinical trials update from the American College of Cardiology meeting 2010: DOSE, ASPIRE, CONNECT, STICH, STOP-AF, CABANA, RACE II, EVEREST II, ACCORD, and NAVIGATOR. Eur J Heart Fail. 2010;12:623-629.
- Calkins H. Catheter ablation of accessory pathways, atrioventricular nodal reentrant tachycardia, and the atrioventricular junction: final results of a prospective, multicenter clinical trial. The Atakr Multicenter Investigators Group. Circulation. 1999;99:262-270.
- Tsai CF, Tai CT, Yu WC, et al. Is 8-mm more effective than 4-mm tip electrode catheter for ablation of typical atrial flutter? Circulation. 1999:100:768-771.
- Piorkowski C, Eitel C, Rolf S, et al. Steerable versus nonsteerable sheath technology in atrial fibrillation ablation: a prospective, randomized study. Circ Arrhythm Electrophysiol. 2011;4(2):157-165.
- Pappone C, Rosanio S, Augello G, et al. Mortality, morbidity, and quality of life after circumferential pulmonary vein ablation for atrial fibrillation: outcomes from a controlled nonrandomized long-term study. J Am Coll Cardiol. 2003;42:185-197.
- Nademanee K, McKenzie J, Kosar E, et al. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004;43:2044-2053.
- Oral H, Scharf C, Chugh A, et al. Catheter ablation for paroxysmal atrial fibrillation: segmental pulmonary vein ostial ablation versus left atrial ablation. Circulation. 2003;108:2355-2360.
- Pappone C, Santinelli V, Manguso F, et al. Pulmonary vein denervation enhances long-term benefit after circumferential ablation for paroxysmal atrial fibrillation. Circulation. 2004;109:327-334.
- Corley SD, Epstein AE, DiMarco JP, et al. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Study. Circulation. 2004;109(12):1509-1513.
- Sanders P, Jaïs P, Hocini M, Haïssaguerre M. Electrical disconnection of the coronary sinus by radiofrequency catheter ablation to isolate a trigger of atrial fibrillation. J Cardiovasc Electrophysiol. 2004;15:364-368.
- Chen SA, Tai CT. Catheter ablation of atrial fibrillation originating from the non-pulmonary vein foci. J Cardiovasc Electrophysiol. 2005;16(2):229-232.
- Packer DL, Keelan P, Munger TM, et al. Clinical presentation, investigation, and management of pulmonary vein stenosis complicating ablation for atrial fibrillation. Circulation. 2005;111(5):546-554.
- Gonzalez MD. Rate control vs. pulmonary vein isolation. Am J Geriatr Cardiol. 2005;14(1):26-30.
- Oral H, Chugh A, Scharf C, et al. Catheter ablation for persistent atrial fibrillation: Segmental pulmonary venous ostial ablation vs. left atrial circumferential ablation, vs. left atrial ablation guided by local electrograms. Circulation. 2003;108:IV-618(A).
- Fisher WG, Swartz JF. Catheter-based three-dimensional electrogram acquisition and analysis system. J Electrocardiol. 1993;26 Suppl:174-181.
- Oral H, Chugh A, Lemola K, et al. Noninducibility of atrial fibrillation as an end point of left atrial circumferential ablation for paroxysmal atrial fibrillation. Circulation. 2004;110:2797-2801.
- Scharf C, Oral H, Chugh A, et al. Acute effects of left atrial radiofrequency ablation on atrial fibrillation. J Cardiovasc Electrophysiol. 2004;15:515-521.
- Pappone C, Oral H, Santinelli V, et al. Atrio-esophageal fistula as a complication of percutaneous transcatheter ablation of atrial fibrillation. Circulation. 2004;109:2724-2726.
- Oral H, Morady F. Ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2004;15:112-113.
- Konings KT, Smeets JL, Penn OC, et al. Configuration of unipolar atrial electrograms during electrically induced atrial fibrillation in humans. Circulation. 1997;95:1231-1241.
- Oral H, Knight B, Ozaydin M, et al. Clinical significance of early recurrences of atrial fibrillation after pulmonary vein isolation. J Am Coll Cardiol. 2002;40(1):100-104.
- Oral H, Knight B, Ozaydin M, et al. Segmental ostial ablation to isolate the pulmonary veins during atrial fibrillation: feasibility and mechanistic insights. Circulation. 2002;106(10):1256-1262.
- Jalife J. Rotors and spiral waves in atrial fibrillation. J Cardiovasc Electrophysiol. 2003;14(7):776-780.

