

Incorporation of Robotic Training into the Traditional EP Fellowship Training Program
Although catheter ablation for atrial fibrillation is one of the most common ablation procedures performed, procedural outcomes remain closely related to operator skill and experience. Manual catheter manipulation can be susceptible to difficulties with catheter stability and ability to maneuver to all sites within the left atrium. Robotic catheter navigation could provide a solution to this. A recent survey suggests that catheter ablation with the robotic system yields a high overall rate of success without an increase in the complication rate, as compared to manual manipulation.1 In this article, we describe our development of a training program that incorporates robotics early in EP fellowship.
About the Technology
 In the United States, the currently available remote navigation systems include Stereotaxis, which is magnet-based, the Hansen Medical Robotic Navigation System, which is electromechanical in nature, and the recently FDA-approved Catheter Robotics’ Amigo Remote Catheter System.
In the United States, the currently available remote navigation systems include Stereotaxis, which is magnet-based, the Hansen Medical Robotic Navigation System, which is electromechanical in nature, and the recently FDA-approved Catheter Robotics’ Amigo Remote Catheter System.
The Hansen system is a flexible, purely robotic platform, which combines three-dimensional catheter control and three-dimensional visualization during procedures. It transfers the hand motions from the physician workstation to the catheter inside the cardiac chambers and provides accurate and easier catheter placement. One of the principal advantages of this technology is that once the catheter reaches the intended site, the robotic system holds the catheter extremely stable. This translates into better tissue contact between the atrial endocardium and the tip of the ablation catheter, and could lead to improved procedural outcomes. In addition, the steerable nature of the robotic sheath also contributes to the stability of the ablation catheter.
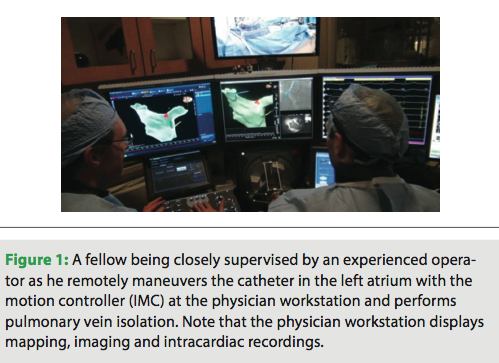
 The Hansen system is comprised of two major components: a physician workstation and the bedside subsystem. The physician workstation is where the operator remotely controls the catheter. It includes three display screens, the Instinctive Motion Controller (IMC), and a control console. The display screens are used to display images from the recording, mapping, and imaging during the procedure. Indicators in the navigational window help display the position of the catheter. The IMC is what allows the physician to remotely control direct catheter movement. Hand movements are copied by the tip of the catheter. The bedside subsystem importantly includes the Remote Catheter Manipulator (RCM), which moves the catheter in response to movements at the IMC from the workstation.
The Hansen system is comprised of two major components: a physician workstation and the bedside subsystem. The physician workstation is where the operator remotely controls the catheter. It includes three display screens, the Instinctive Motion Controller (IMC), and a control console. The display screens are used to display images from the recording, mapping, and imaging during the procedure. Indicators in the navigational window help display the position of the catheter. The IMC is what allows the physician to remotely control direct catheter movement. Hand movements are copied by the tip of the catheter. The bedside subsystem importantly includes the Remote Catheter Manipulator (RCM), which moves the catheter in response to movements at the IMC from the workstation.
Experience at Our Institution
Since the Hansen Medical Robotic Navigation System at the University of Virginia (UVA) was installed in 2008, we have performed over 200 robotic cases with the vast majority being complex left atrial procedures. With a robust procedure-based fellowship as well as increasing evidence of potentially improved tissue contact and enhanced catheter stability in ablation procedures, a growing number of fellows coming through the training program are expressing interest in incorporating robotic training into their EP fellowship.
At most EP institutions with robotic systems in place, training usually focuses on fellows attaining manual skills before training on the robot. However, there is no data within electrophysiology that has examined whether this traditional approach to training is the best approach. At our current two-year training program, we are developing a curriculum in which fellows are simultaneously trained both manually and robotically. This is in contrast to most other programs in the U.S., but we have data from our institution that would support this method.
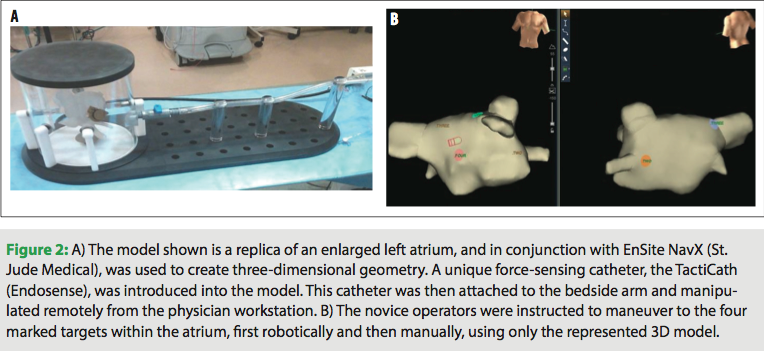
In an attempt to prove that proficiency in manual skills prior to robotic training is not necessary, we enrolled novice medical professionals, people who had had no prior catheter experience at all, and assessed their ability to manipulate catheters both robotically and manually. An in vitro setup consisted of a synthetic model of the left atrium, into which a unique force-sensing catheter, the TactiCath (Endosense), was introduced. This catheter was then attached to the bedside arm and manipulated remotely from the physician workstation. For manual manipulation, an Agilis sheath (St. Jude Medical) was used to help steer the catheter. Using a three-dimensional geometry created with EnSite NavX (St. Jude Medical), operators had to maneuver to four points in successive order and achieve a contact force of 20–40 grams using feedback from the TactiCath: anteriorly in the left superior pulmonary vein (LSPV), posteriorly in the left inferior pulmonary vein (LIPV), posteriorly in the right superior pulmonary vein (RSPV), and then anteriorly in the right inferior pulmonary vein (RIPV).2 Additionally, we monitored for areas of excessive force, defined as greater than 100 grams.3
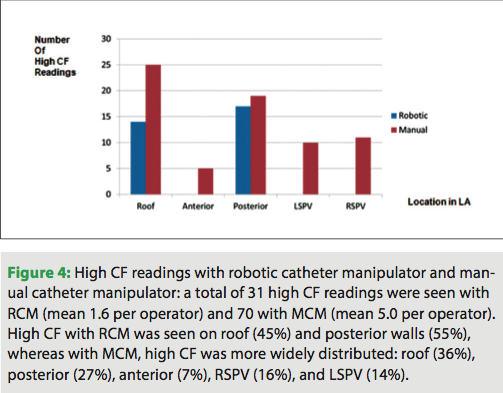
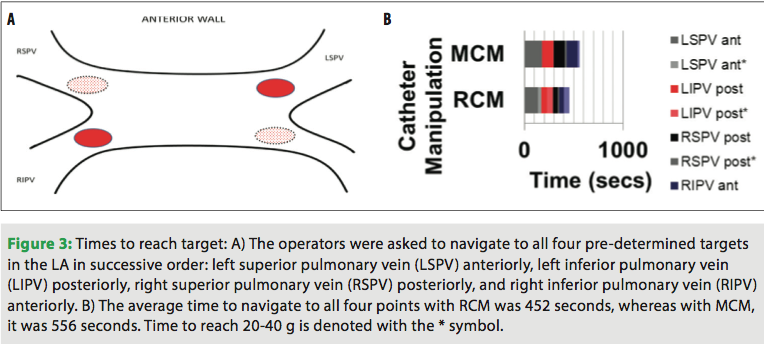 Twenty subjects participated in the evaluation. In a post-study questionnaire, the majority of participants (85%) reported that robotic manipulation was easier than manual manipulation. In addition, times to reach all four pre-designated points and achieve adequate contact were shorter in the robotic arm than the manual arm (Figure 3). There were also significantly fewer episodes of excessive force with robotic manipulation as well (Figure 4). We could infer from these results that training on the robotic system does not require prior expertise in manual catheter manipulation, does not lead to excessive procedural times, and is actually associated with fewer episodes of excessive force, which could enhance safety for novice users.
Twenty subjects participated in the evaluation. In a post-study questionnaire, the majority of participants (85%) reported that robotic manipulation was easier than manual manipulation. In addition, times to reach all four pre-designated points and achieve adequate contact were shorter in the robotic arm than the manual arm (Figure 3). There were also significantly fewer episodes of excessive force with robotic manipulation as well (Figure 4). We could infer from these results that training on the robotic system does not require prior expertise in manual catheter manipulation, does not lead to excessive procedural times, and is actually associated with fewer episodes of excessive force, which could enhance safety for novice users.
 Most of our previous understanding of training in robotics comes largely from surgical data. There is a great paucity of such research in the field of electrophysiology. Since the advent of the da Vinci robot in surgical sub-specialties, it has become so widely used that training in robotics has become a necessity in surgical residencies and fellowships. In response to growing concerns several years ago that most surgeons performing robotic procedures were inadequately trained, a taskforce was convened, the primary purpose of which was to help define a more standard curriculum for training in surgical robotics. Many of their principles can be applied to an EP fellowship training program in which a robotic system is available, but we have yet to develop our own such standardized teaching curriculum.
Most of our previous understanding of training in robotics comes largely from surgical data. There is a great paucity of such research in the field of electrophysiology. Since the advent of the da Vinci robot in surgical sub-specialties, it has become so widely used that training in robotics has become a necessity in surgical residencies and fellowships. In response to growing concerns several years ago that most surgeons performing robotic procedures were inadequately trained, a taskforce was convened, the primary purpose of which was to help define a more standard curriculum for training in surgical robotics. Many of their principles can be applied to an EP fellowship training program in which a robotic system is available, but we have yet to develop our own such standardized teaching curriculum.
At our institution, we are in the process of developing a training program that incorporates robotics early in the fellowship. Incoming EP fellows are now being trained simultaneously on the Hansen system, while at the same time still developing manual skills. The fellows start with an introduction to the system and its components, with the help of clinical staff from Hansen Medical. Fellows observe cases being performed by an experienced operator, the attending, and also have the opportunity to practice on the simulator. Then, in a step-wise fashion, they begin performing parts of the procedure while being supervised, and as they progress, become increasingly independent.
In addition to the training of fellows, training of the lab staff also remains crucial. The smooth functioning of a case using the robotic system relies on a well-trained and supportive group of staff, technicians and nurses. Our lab technicians and nurses have been carefully trained and are familiar with all system components of the Hansen robot. They have become proficient in setup of the system and are able to efficiently troubleshoot when any issues arise. A well-trained team helps positively affect the performance of the operator.
Summary
Ablation procedures for atrial fibrillation are becoming increasingly common, and while success rates at experienced centers are high, recurrences still occur. Robotic catheter manipulation can help overcome issues with catheter stability and difficult maneuverability. This could lead to improved ablation lesions, with less recovery of conduction and thus, fewer recurrences. With the increasing evidence supporting the use of robotics in catheter ablation, for the current generation of fellows who are fortunate enough to train at an institution with such a system, integration of robotic training into the fellowship program would be advantageous. We believe that attainment of manual skills prior to initiation of robotic training is not necessary. In contrast, we support the strategy of simultaneous manual and robotic training, with early incorporation of robotics into an EP fellowship program.
Disclosures: Dr. Hussain has no conflicts of interest to report. Dr. Mangrum reports consultancy, honoraria, and payment for development of educational presentations including service on speakers’ bureaus from St. Jude Medical; he also reports grants/grants pending from St. Jude Medical, Hansen Medical, and Endosense.
References
- Bai R, Di Biase L, Valderrabano M, et al. Worldwide experience with the robotic navigation system in catheter ablation of atrial fibrillation: Methodology, efficacy and safety. J Cardiovasc Electrophysiol. 2012;23(8):820-826.
- Reddy VY, Shah D, Kautzner J, et al. The relationship between contact force and clinical outcome during radiofrequency catheter ablation of atrial fibrillation in the TOCCATA study. Heart Rhythm. 2012;9(11):1789-1795.
- Shah D, Lambert H, Langenkamp A, et al. Catheter tip force required for mechanical perforation of porcine cardiac chambers. Europace. 2011;13(2):277-283.

