

ADVERTISEMENT
Hybrid EP Labs: A Growing Trend
 Hybrid ORs were born out of a need for vascular surgeons to be able to do minimally invasive and invasive surgical procedures utilizing advanced X-ray techniques. Accordingly, their most widespread use is for vascular procedures. However, as the sheer volume of electrophysiology procedures increases, hybrid EP labs are becoming more common.
Hybrid ORs were born out of a need for vascular surgeons to be able to do minimally invasive and invasive surgical procedures utilizing advanced X-ray techniques. Accordingly, their most widespread use is for vascular procedures. However, as the sheer volume of electrophysiology procedures increases, hybrid EP labs are becoming more common.
A hybrid EP lab has the capability to perform a range of procedures — from complex to minimally invasive — all within the same room. This means an EP procedure can seamlessly transition into an invasive procedure should complications arise. The ability to transition from non-invasive to more invasive procedures within the same operating space provides significant benefits, including improved safety for the patient and increased efficiency for the hospital.
Hybrid ORs represent new capabilities for hospitals, and the number of facilities moving toward a multidisciplinary operating space is growing. As electrophysiologists increasingly need to perform complex cardiac procedures, hybrid ORs are rapidly becoming an important resource for EP programs.
Impact on Patient Safety
The features of a hybrid EP lab can have a dramatic impact on the safety profile of a procedure, contributing to better outcomes and patient safety. Hybrid EP labs are an ideal setting to provide a range of services for patients that would ordinarily need more than one procedure to address their condition.
In traditional EP lab settings, if a cardiovascular patient developed a complication during surgery, the patient would need to be moved to an operative setting in a critically unstable condition. Due to the time it takes to move a patient to a different procedure room, there is a high risk of exposing the patient to additional risk, infection, or a prolonged procedure. A multidiscipline hybrid EP lab eliminates the need to move from room to room and along with it, the associated risk.
Expanded Procedure Options for Physicians
 In a hybrid EP lab, physicians have the full range of equipment necessary to change the scope of a procedure from minimally invasive to more invasive as needed. In addition, the full suite of equipment in a hybrid EP lab, including recording and mapping systems as well as advanced imaging modalities to support procedures with interventional cardiology crossover, also allows physicians to perform multiple procedures simultaneously or back-to-back.
In a hybrid EP lab, physicians have the full range of equipment necessary to change the scope of a procedure from minimally invasive to more invasive as needed. In addition, the full suite of equipment in a hybrid EP lab, including recording and mapping systems as well as advanced imaging modalities to support procedures with interventional cardiology crossover, also allows physicians to perform multiple procedures simultaneously or back-to-back.
Hybrid EP labs are outfitted with anesthesia equipment, angiographic suite equipment, equipment booms, and ample space. Collectively, these features allow physicians to execute emergency procedures that ultimately help to minimize complications or decrease morbidity and mortality for patients.
In the past, there were certain procedures only performed by cardiologists and certain procedures only performed by cardiothoracic surgeons. Electrophysiology is a good example of crossing boundaries between these two disciplines and, essentially, is where a hybrid OR offers the best of both worlds. For example, at UC Irvine, adult patients with congenital heart defects that require multiple procedures can be evaluated and treated using a team approach in one scheduled procedure.
Planning and Building Considerations
 The University of California, Irvine Medical Center, a 322-bed facility in Orange County, California, was an early adopter of the hybrid OR concept. When its state-of-the-art hospital was built in 2009, two of the 22 operating rooms were constructed as hybrid ORs: a vascular hybrid OR and a hybrid EP lab. Since the opening of the hybrid EP lab in January 2011, over 350 procedures have been performed in the 750 square foot room. The space has been utilized for the whole spectrum of EP, cardiac, and vascular surgery cases; perioperative services and cardiovascular services attribute the success of the multi-use model to a teamwork philosophy that was adopted by physicians, leadership and the staff that are directly involved in providing direct clinical care.
The University of California, Irvine Medical Center, a 322-bed facility in Orange County, California, was an early adopter of the hybrid OR concept. When its state-of-the-art hospital was built in 2009, two of the 22 operating rooms were constructed as hybrid ORs: a vascular hybrid OR and a hybrid EP lab. Since the opening of the hybrid EP lab in January 2011, over 350 procedures have been performed in the 750 square foot room. The space has been utilized for the whole spectrum of EP, cardiac, and vascular surgery cases; perioperative services and cardiovascular services attribute the success of the multi-use model to a teamwork philosophy that was adopted by physicians, leadership and the staff that are directly involved in providing direct clinical care.
Because hybrid ORs allow for more disciplines to utilize the same space, there are unique and substantial planning considerations that must be taken into account in order to ensure that the space is optimized and intuitive for each discipline.
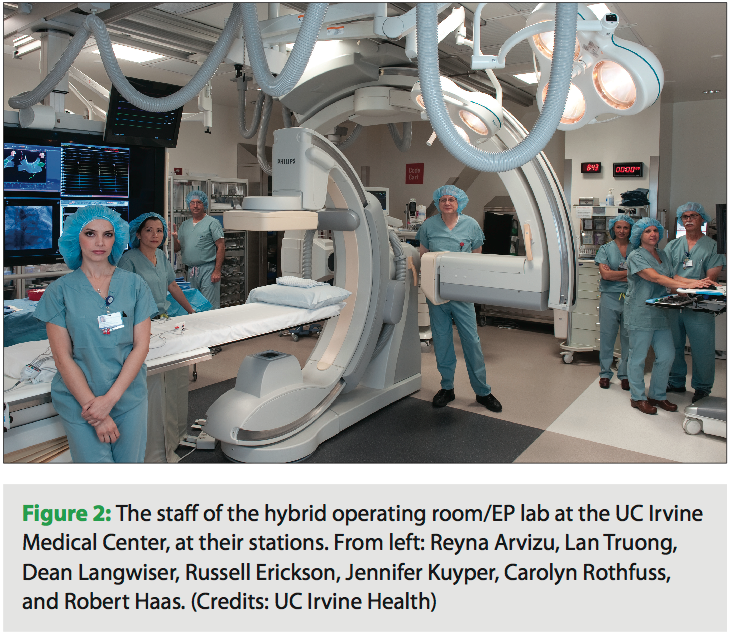
Some of the many considerations include ventilation and air exchange requirements, traffic around sterile fields, bringing gas and electricity into the room, storage for equipment (especially disposables), locations for the EP cockpit, EP equipment boom, anesthesia boom, and supplies, OR and cath lab documentation stations, nursing supplies and medication storage, locations for IT and phone lines, refrigerator, and crash cart and defibrillator. Major considerations such as fluoroscopy and fluoroscopy exposure also need to be well planned, including the location and number of ceiling-mounted radiation shields as well as location and size of mobile radiation shields. Another major consideration that can be easily overlooked is outfitting the hybrid OR with the better quality surgical lights; the highest quality surgical lights are a very important tool for surgeons, and should be planned for in the hybrid EP suite.
An integral part of the planning and design process is a team of people willing to work together. The amount of equipment being installed often creates competing themes between different disciplines in terms of what is necessary. At UC Irvine, the OR, cardiology, cath lab, and EP lab managers were all involved at a hands-on level in the planning and design process.
UC Irvine scheduled regular meetings on the project that truly touched every stakeholder: cardiac surgeons, vascular surgeons, cardiologists, interventional cardiologists, EP cardiologists, radiology technicians, vendors and their clinical engineers, physician operators, nurses and support staff. Architectural meetings started two years prior, and installation of equipment meetings started one year prior to opening. Molly Nunez, RN, MSN, ACNP, nurse manager of the cardiac cath and EP labs at UC Irvine, explains, “It’s imperative to have everybody in the same room to ask, Is there a problem if we do this? You can’t meet with the vendors separately and plan the installations.”
Tips for the Hybrid OR Space
Given the extensive thought process that goes into planning and designing a hybrid OR, here are some of the insights we have learned at UC Irvine:
- Have a multidisciplinary approach in terms of physical design. Consult the staff who will be working in the new space in order to avoid conflict. Operations are an important part of planning and should be considered early in the process.
- Overall logistics regarding the location of equipment, access to physicians and the ability to communicate should be discussed and carefully considered upfront. Understanding who needs to interact with each other and getting early input will provide invaluable input for planning purposes.
- Another consideration is whether the control room should be shared with another OR, which can save space, but can also introduce additional distractions for staff.
- Invest in equipment booms. It may be an expensive investment, but there is a big push right now in EP and interventional cardiology services for changes in paradigm about infectious disease standards.
- Hard install equipment. The nature of an EP procedure involves having many metal objects around, and if the location of metal within the room is changed, there is the chance it can affect procedures and the performance of the equipment and technology. Hard installs eliminate this variable.
- If possible, install new equipment. A true hybrid OR space can cost up to $4M. However, the average life of equipment is seven years — new equipment ensures better connectivity between systems and better video resolution.
Making the Business Case
 Hybrid ORs create efficiency throughput — saving both time and space. A key financial benefit for the hospital also lies in having multiple uses for the space. Since a hybrid EP lab houses multidisciplinary equipment, when the space isn’t being used for EP lab procedures, other types of cases can be performed; at UCI, the room is set up to perform comprehensive interventional cardiology cases, but is also used for vascular, endovascular, interventional radiology, and AAA cases during downtime.
Hybrid ORs create efficiency throughput — saving both time and space. A key financial benefit for the hospital also lies in having multiple uses for the space. Since a hybrid EP lab houses multidisciplinary equipment, when the space isn’t being used for EP lab procedures, other types of cases can be performed; at UCI, the room is set up to perform comprehensive interventional cardiology cases, but is also used for vascular, endovascular, interventional radiology, and AAA cases during downtime.
When soliciting approval or buy-in from upper management for a hybrid OR, it often comes down to making a strong business case. “We looked at our business strategies and our priorities, and we wanted to build our EP program as the best in the region. At the same time, we knew our vascular services were planning to become an AAA receiving center. Both medicine and surgical physician leadership presented compelling cases for the space and making the investment. Even though these rooms were more expensive to build, it made sense in order to achieve our business goals,” said Nunez.
Financial benefits are an ever-changing dynamic because these cost centers, codes, and amounts are moving targets. Many EP lab procedures are not typical “bread and butter” procedures for a hospital, but there are some unique opportunities that a hybrid room can allow hospitals to capitalize on, such as transcatheter aortic valve replacements that may require EP interventions.
A hybrid EP lab expands the capabilities of the hospital. This combination of expanded capabilities and the increase in the volume of procedures the lab can perform translates into income that can be used to help offset costs. Ultimately, complications are expensive, so increasing efficiency and patient safety is key to minimizing complications and offsetting costs.
Higher volume centers will also be able to easily demonstrate improved efficiency and therefore experience a real cost benefit in the adoption of a hybrid lab.
Experience at UCI
The biggest impact of hybrid EP labs is on patient safety standards, which are at a much higher level today than they were even ten years ago.
The hybrid EP lab allows us to transition from a less invasive to a more invasive procedure on the fly based solely on patient needs and not logistics. This ability to transition quickly provides a level of security for me as a physician and translates to better outcomes for my patients.
There is also an increased level of patient care found within a hybrid OR thanks to cross-disciplinary training within the hospital’s ancillary staff and team of allied professionals.
I have resigned practicing privileges from hospitals simply because they either lacked equipment or facilities. If you have the bare minimum equipment, you’re doing the bare minimum procedures; the simplest catheter ablation or the simplest device implant is done in the basic cath lab or basic OR. The utilization of a hybrid room allows for more complex procedures that may be more risky, but are higher-end procedures.
The ease-of-use in a hybrid OR is vastly improved and having everything contained in one environment is a huge help, but the primary advantage, in my opinion, is in the capabilities of these facilities. From a bottom-line standpoint, I think procedures are safer in a hybrid OR setting.
The Future of Hybrid ORs
 There is no doubt hybrid ORs will increase in prevalence, as they present new opportunities to cardiologists and the industry at large. EP techniques and procedures are evolving, and having the resources available to execute them becomes crucial to make the job easier and faster.
There is no doubt hybrid ORs will increase in prevalence, as they present new opportunities to cardiologists and the industry at large. EP techniques and procedures are evolving, and having the resources available to execute them becomes crucial to make the job easier and faster.
For EPs today, techniques including left atrial appendage occlusion can result in an emergent situation that would require a physician to convert to an open procedure, but in the right situation, the preference may actually be to do an open procedure first. Having the ability to seamlessly transition strategy or treatment is incredibly important for these higher-end procedures. Another emerging procedure is hybrid AF ablation, and the combination of a surgical fluoroscopic technique and catheter ablation is only found in a hybrid room. More advanced procedures will be widely adopted in the future, and hybrid EP labs will play an important role in this future due to their ability to serve multiple disciplines within the cardiovascular space.
Hybrid OR use is growing, and in the meantime, hospitals can use the availability of a hybrid EP lab as a marketing differentiator to attract both patients and physicians.
Take a virtual tour of UC Irvine’s hybrid EP lab by visiting:
https://www.healthcare.uci.edu/
virtualtours/standalones/hybrid_or/tourfiles/flash/index.html

