

Expert Roundtable Fills in Vital Pieces of Afib Treatment Puzzle: The Afib Optimal Treatment Task Force and the Expert Working Group
 For some healthcare professionals, treating afib can be a little like figuring out a jigsaw puzzle. Pieces here and there provide clues about the overall picture, but seeing the whole picture and being able to assemble a treatment regimen is a bit more difficult. And just like a puzzle is easier with several hands helping, developing an afib treatment plan has become less complicated through the work of the Afib Optimal Treatment Task Force and the Expert Working Group.
For some healthcare professionals, treating afib can be a little like figuring out a jigsaw puzzle. Pieces here and there provide clues about the overall picture, but seeing the whole picture and being able to assemble a treatment regimen is a bit more difficult. And just like a puzzle is easier with several hands helping, developing an afib treatment plan has become less complicated through the work of the Afib Optimal Treatment Task Force and the Expert Working Group.
The Afib Optimal Treatment Task Force, led by the Alliance for Aging Research, convened an expert roundtable to discuss strategies for risk assessment and treatment to prevent afib-related strokes. StopAfib.org was a member of the task force, and as founder, I represented the afib patient community on the expert roundtable. The group focused on the underutilization of anticoagulants for afib patients. Anticoagulants are effective at preventing strokes in afib patients, yet a large percentage of afib patients don’t receive these potentially lifesaving medications.
“The Alliance for Aging Research Consensus Statement on Appropriate Anticoagulant Use addresses a very important and unmet need in the elderly population, namely, the inadequate use of antithrombotic prophylaxis in patients at risk for stroke with atrial fibrillation,” said Dr. Albert L. Waldo, one of the authors of the consensus statement. “Study after study has shown that despite the absence of contraindications to oral anticoagulant therapy, only 40 to 60 percent of patients with a significant risk for stroke in the presence of atrial fibrillation receives anticoagulation therapy, and the patients least likely to receive it are the most elderly.”
Dr. Waldo added, “This white paper should go a long way toward helping healthcare professionals provide patients with the care needed to prevent stroke in this growing, at-risk population.”
The group found that anticoagulants may be underused because of doctors’ misperceptions about the clinical benefit of anticoagulant therapy, lack of incentives, time constraints, and lack of specificity about contraindications.
As part of the recommendations, the roundtable assembled stroke and bleeding risk assessment tools.
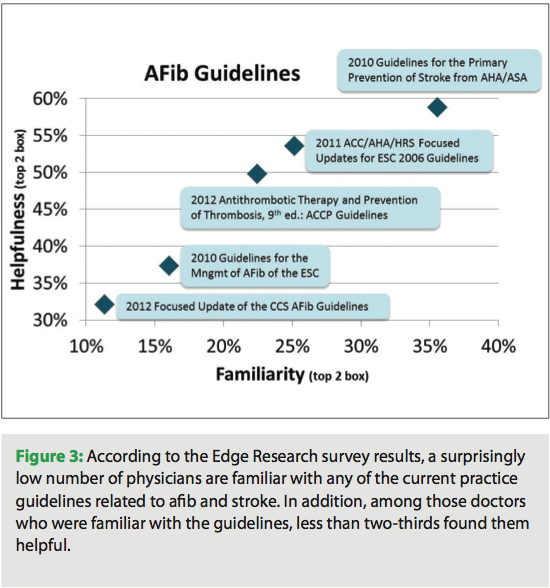
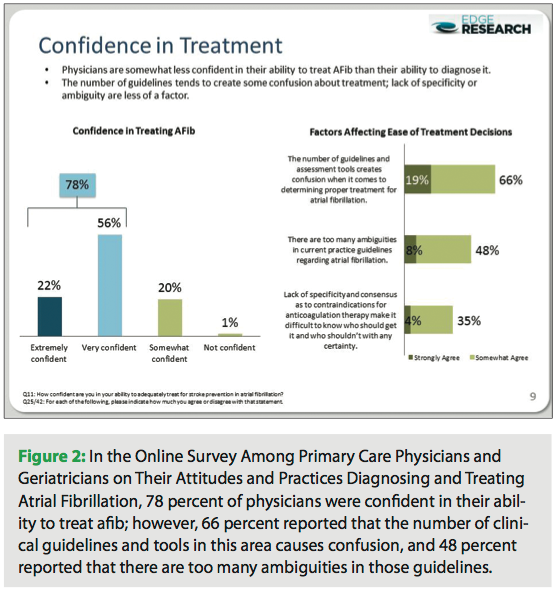 The Alliance also conducted an online survey among primary care physicians and geriatricians about their attitudes and practices in diagnosing and treating afib. The survey was conducted by Edge Research on behalf of the Alliance and the Afib Optimal Treatment Task Force. The results of the survey provided insight about healthcare providers’ assessment and treatment decisions. To access the expert consensus report and the survey results, visit bit.ly/NkhByR.
The Alliance also conducted an online survey among primary care physicians and geriatricians about their attitudes and practices in diagnosing and treating afib. The survey was conducted by Edge Research on behalf of the Alliance and the Afib Optimal Treatment Task Force. The results of the survey provided insight about healthcare providers’ assessment and treatment decisions. To access the expert consensus report and the survey results, visit bit.ly/NkhByR.
“Having this consensus will help reduce confusion and help us make real progress in identifying at-risk individuals and improving the quality and effectiveness of afib treatment,” said Daniel P. Perry, president and CEO of the Alliance. “The survey results and recommendations outlined in the consensus statement highlight the need for increased awareness and consensus surrounding risk assessment and the appropriate use of anticoagulants.”
One of the most dramatic aspects of the group’s recommendations, though, was the incorporation of patients’ opinions and concerns into treatment decisions. To me, this was like putting together all the edge pieces to frame the afib puzzle.
To help healthcare providers understand the group’s findings, here are some of the key recommendations:
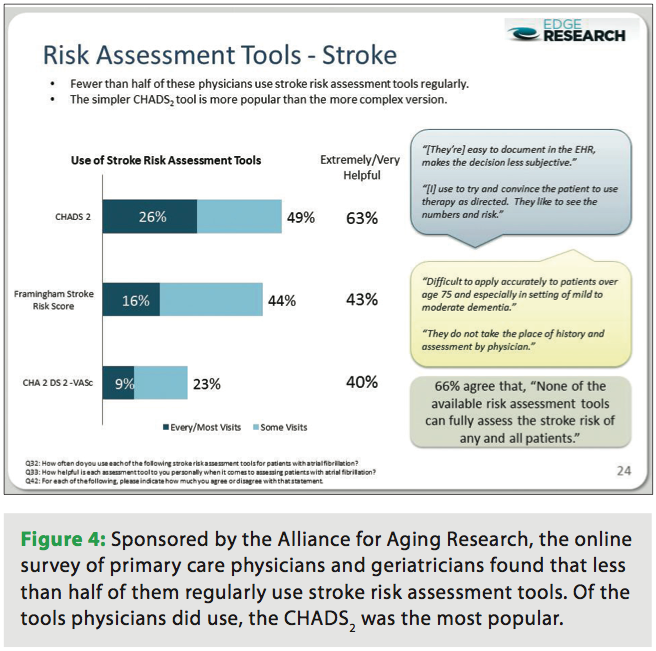
 Use assessment tools. The group compiled a set of easy-to-access stroke and bleeding risk tools for healthcare professionals. These tools include the CHADS2, CHA2DS2-VASc, and Framingham Stroke Risk Score for assessing stroke risk for patients with afib, and HAS-BLED, ATRIA, HEMORR2HAGES, and the Outpatient Bleeding Risk Index (OBRI) for assessing bleeding risk. Within the group’s report, healthcare professionals can find all of these tools in one place.
Use assessment tools. The group compiled a set of easy-to-access stroke and bleeding risk tools for healthcare professionals. These tools include the CHADS2, CHA2DS2-VASc, and Framingham Stroke Risk Score for assessing stroke risk for patients with afib, and HAS-BLED, ATRIA, HEMORR2HAGES, and the Outpatient Bleeding Risk Index (OBRI) for assessing bleeding risk. Within the group’s report, healthcare professionals can find all of these tools in one place.- Assess risk once a year. In addition to providing the stroke risk tools, the group recommended that healthcare professionals annually assess and document in patient charts or EHRs their afib patients’ stroke risk.
- Use anticoagulants for those at intermediate or high risk of stroke. Afib patients who are determined to be at an intermediate or high risk of stroke should be put on an anticoagulant — warfarin or a new agent, such as a direct thrombin inhibitor or a Factor Xa inhibitor.
- Aspirin not recommended. In a groundbreaking recommendation, the roundtable recommended that aspirin not be used for stroke prevention in afib. This new recommendation indicated a novel direction for treatment as it had not been mentioned previously in the guidelines. The roundtable noted that aspirin is less effective than warfarin yet has the potential for bleeding.
- Establish bleeding risk. For patients who require anticoagulation therapy, assess the bleeding risk using a scoring tool to determine the net clinical benefit of use of an anticoagulant medication. Other risk factors, such as uncontrolled hypertension, small vessel disease, dementia, and patients with coronary artery disease who are on antiplatelet therapy should also be considered.
- Balance risk of stroke vs. bleeding. Throughout the discussions, the roundtable acknowledged that deciding whether to anticoagulate can be challenging for doctors. The group found that the fear of bleeding risk from anticoagulants for elderly patients who may fall and suffer a hemorrhage may be exaggerated, as the risk of ischemic stroke without anticoagulants is greater than the risk of intracranial hemorrhage with them. Thus, bleeding risk shouldn’t be used as an excuse to avoid anticoagulating a patient.
- Correct bleeding risk factors. Address correctable bleeding risk factors for patients who require anticoagulation therapy. Some of these correctable factors include hypertension, anemia, renal impairment, labile INRs, use of aspirin or NSAIDs, ethanol abuse, and excessive fall risk.
- Promote patient education. The group found that many patients are unaware that afib increases stroke risk by five times. Healthcare providers should initiate stroke prevention discussions with afib patients, and the roundtable also urged development of initiatives to prompt afib patients to ask about stroke prevention.
- Reflect patients’ preferences and values. As a crucial, major recommendation, the group recommended that healthcare providers be sure that patients understand the benefits and risks of various treatment options. Patients should directly participate in treatment decisions, such as whether to go on anticoagulants and which ones may work the best.
- Increase healthcare provider afib education. The roundtable participants recommended that education and tools at the primary care and family practitioner levels be enhanced. These could include stroke risk assessment tools in EMR systems, awareness activities and events at medical centers, educational initiatives by payers, pocket guides, incentives, and online resources. The need for this information and education was made clear through the survey.
- Continually collect and update afib information. Roundtable participants also agreed that priority should be given to collecting and analyzing real-world data on new anticoagulants to identify which patients are best suited for specific agents.
Good Timing: September is Afib Month
 The roundtable recommendations come at an exciting time for healthcare providers and others working to improve care for afib patients. September is Atrial Fibrillation Awareness Month, which is officially recognized nationally in the United States. Atrial Fibrillation Awareness Month is a time for healthcare providers across the world to educate patients and colleagues about the risk of afib-related strokes, which can be avoided through assessing risk factors with tools mentioned in the roundtable recommendations.
The roundtable recommendations come at an exciting time for healthcare providers and others working to improve care for afib patients. September is Atrial Fibrillation Awareness Month, which is officially recognized nationally in the United States. Atrial Fibrillation Awareness Month is a time for healthcare providers across the world to educate patients and colleagues about the risk of afib-related strokes, which can be avoided through assessing risk factors with tools mentioned in the roundtable recommendations.
In addition to spreading the word about afib, healthcare providers, patients, and others affected by afib can sign the Global Atrial Fibrillation Patient Charter to raise awareness of afib around the globe and ask others to do so, too. It’s easy enough to share the link to the Charter – just post, tweet, or email a link to signagainststroke.com.
To see another recent article by Mellanie True Hills, please visit: https://eplabdigest.com/articles/Global-Atrial-Fibrillation-Patient-Charter-and-Sign-Against-Stroke-Atrial-Fibrillation-Camp
