

Endurance Exercise: Is it Proarrhythmic?
 Like many people in the healthcare field, I took to running as a hobby that could fit around a busy practice and that had many health benefits and rewards. I completed my sixth marathon, the Philadelphia Marathon, in November 2011 in good spirits, not knowing that two participants had died suddenly that day. Jeffrey Lee, a 21-year-old nursing student, died just after finishing the half marathon.
Like many people in the healthcare field, I took to running as a hobby that could fit around a busy practice and that had many health benefits and rewards. I completed my sixth marathon, the Philadelphia Marathon, in November 2011 in good spirits, not knowing that two participants had died suddenly that day. Jeffrey Lee, a 21-year-old nursing student, died just after finishing the half marathon.
Chris Gleason, a 40-year-old accomplished Ironman triathlete, died almost within sight of the marathon finish. In the November 2012 issue of Runner’s World magazine, Peter Sagal of National Public Radio and also a marathoner, wrote an appreciation of Chris Gleason.1 In the article, it states that after autopsy and toxicology results, his death was attributed to an “unspecified cardiomyopathy.” These deaths and an awareness of some recent literature about adverse cardiovascular effects of endurance exercise led me to take a closer look at this literature. I will summarize what I have learned, especially as it pertains to arrhythmias, in the following paragraphs.
Sudden Death During Marathons
For many years we have understood that strenuous, prolonged exercise such as a marathon may trigger cardiac arrest and sudden death, typically from ventricular fibrillation, in occasional athletes, and almost always men. The risk was recently estimated at 1 to 2 per 100,000 marathon participants.2 We have understood that the risk relates to the combination of a trigger, being the major hemodynamic, autonomic, electrolyte and other changes happening during and on cessation of the effort, and a substrate, which is a previously unidentified heart disease. The type of underlying heart disease breaks down according to age; in those younger than about 35 years it is usually a congenital problem such as hypertrophic cardiomyopathy, and in those over 35 years it is usually coronary artery disease. This remains a valid hypothesis and appears to explain most deaths.2 This hypothesis leads to efforts to identify those with at-risk structural heart disease prior to participation and to improve resuscitation efficacy during events, as well as other ways to prevent these rare but tragic deaths.3 This is an increasingly important issue as more adults exercise and participate in mass running events.
Potential Adverse Cardiovascular Effects From Excessive Endurance Exercise
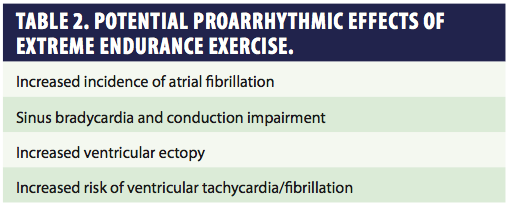
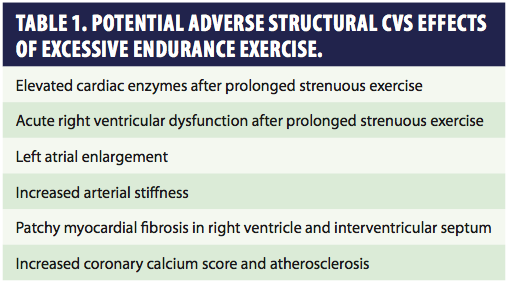 In the scenario of sudden death during marathons and triathlons, the exercise has been considered simply a trigger of ventricular arrhythmia, the underlying heart disease being present, unrecognized and not due to the exercise per se. We have a wealth of observational data that regular, moderate exercise reduces the risk of coronary events and prolongs life. However, as I reviewed the recent literature I find concerns that excessive endurance exercise, especially for men in middle age and later in life, might actually increase the risk of cardiovascular disease. These potential adverse structural changes in the heart and vasculature are summarized in Table 1 and are excellently reviewed by Dr. James O’ Keefe and colleagues.4 These structural changes provide a possible substrate for atrial and ventricular arrhythmias, both bradycardia and tachycardia. I will focus on these potential proarrhythmic effects of excessive endurance exercise, summarized in Table 2.
In the scenario of sudden death during marathons and triathlons, the exercise has been considered simply a trigger of ventricular arrhythmia, the underlying heart disease being present, unrecognized and not due to the exercise per se. We have a wealth of observational data that regular, moderate exercise reduces the risk of coronary events and prolongs life. However, as I reviewed the recent literature I find concerns that excessive endurance exercise, especially for men in middle age and later in life, might actually increase the risk of cardiovascular disease. These potential adverse structural changes in the heart and vasculature are summarized in Table 1 and are excellently reviewed by Dr. James O’ Keefe and colleagues.4 These structural changes provide a possible substrate for atrial and ventricular arrhythmias, both bradycardia and tachycardia. I will focus on these potential proarrhythmic effects of excessive endurance exercise, summarized in Table 2.
Increased Incidence of Atrial Fibrillation
 There is now very strong epidemiologic data that prolonged endurance exercise is associated with an increased risk of atrial fibrillation, anywhere from a 2- to 10-fold increase in long-term endurance athletes compared to sedentary controls.5,6 I suspect that all of us in cardiac electrophysiology have seen middle-aged and older men with paroxysmal atrial fibrillation (PAF) who are otherwise healthy and have remained very physically active for many years with endurance sports, often running. Their PAF is usually quite symptomatic, not necessarily occurring during exercise but more often at night, as has been reported for “vagal” PAF. There is almost always co-existing sinus bradycardia at rest, which makes the treatment of PAF very difficult. A number of mechanisms have been suggested to increase the risk of atrial
There is now very strong epidemiologic data that prolonged endurance exercise is associated with an increased risk of atrial fibrillation, anywhere from a 2- to 10-fold increase in long-term endurance athletes compared to sedentary controls.5,6 I suspect that all of us in cardiac electrophysiology have seen middle-aged and older men with paroxysmal atrial fibrillation (PAF) who are otherwise healthy and have remained very physically active for many years with endurance sports, often running. Their PAF is usually quite symptomatic, not necessarily occurring during exercise but more often at night, as has been reported for “vagal” PAF. There is almost always co-existing sinus bradycardia at rest, which makes the treatment of PAF very difficult. A number of mechanisms have been suggested to increase the risk of atrial 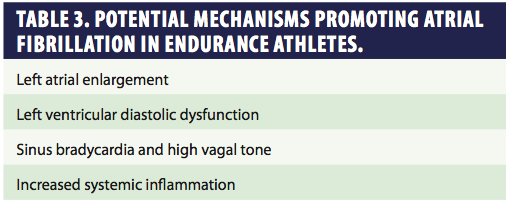 fibrillation in older athletes, and these are outlined in Table 3. In my opinion, the evidence points to atrial enlargement, probably compounded by high vagal tone and possibly increased inflammation as the mechanisms driving PAF in older athletes.5,6 Atrial enlargement and possibly atrial fibrosis likely occur due to repeated high output demands and maybe subtle ventricular diastolic dysfunction.4,5 Currently we do not know how to predict which athletes may be at risk for PAF, or if exercise cessation or reduced training would lead to a resolution of PAF. We treat these patients like other PAF patients, but usually rhythm control is the preferred strategy because of symptoms. Anecdotally, I use flecainide as an initial antiarrhythmic drug since I find that it is often effective in suppressing PAF and symptomatic atrial ectopy in these patients without exacerbating bradycardia. Catheter ablation with pulmonary venous isolation, in my view, is an excellent option for treatment of PAF in endurance athletes, and the reported results match those of other PAF patients.7,8
fibrillation in older athletes, and these are outlined in Table 3. In my opinion, the evidence points to atrial enlargement, probably compounded by high vagal tone and possibly increased inflammation as the mechanisms driving PAF in older athletes.5,6 Atrial enlargement and possibly atrial fibrosis likely occur due to repeated high output demands and maybe subtle ventricular diastolic dysfunction.4,5 Currently we do not know how to predict which athletes may be at risk for PAF, or if exercise cessation or reduced training would lead to a resolution of PAF. We treat these patients like other PAF patients, but usually rhythm control is the preferred strategy because of symptoms. Anecdotally, I use flecainide as an initial antiarrhythmic drug since I find that it is often effective in suppressing PAF and symptomatic atrial ectopy in these patients without exacerbating bradycardia. Catheter ablation with pulmonary venous isolation, in my view, is an excellent option for treatment of PAF in endurance athletes, and the reported results match those of other PAF patients.7,8
Sinus Bradycardia and Conduction Impairment
Resting sinus bradycardia and associated conduction disturbances are well recognized in the young athlete and have long been considered benign. My concern is when we still see profound sinus bradycardia associated with endurance exercise persisting into later life. In current electrophysiology practice, we are often consulted about the need for pacing in these middle-aged and older individuals, typically men. Most individuals appear asymptomatic and thus do not have a pacing indication, but anecdotally, we have seen a minority who appear to develop symptomatic bradycardia and require pacing, as has been reported in the literature.9 One could speculate that these occasional cases represent a combination of the normal age-related changes in the conduction system occurring on top of the vagal or other chronic effects of endurance exercise. Such cases remain rare, but some concern has recently been raised about the effects of chronic bradycardia on the vasculature. Because bradycardia is associated with a higher stroke volume and a higher pulse pressure, over many years these may contribute to increased arterial stiffness and abnormal vascular remodeling.10
Increased Ventricular Arrhythmia
There have been reports of a minority of endurance athletes developing symptomatic ventricular ectopy in the absence of obvious structural heart disease. Again, the phenomenon has been described in middle-aged men, typically runners. We have seen such cases in our own electrophysiology practice. In this scenario, there is data that a period of exercise cessation or marked reduction in training results in a reduction of ectopy.11 These cases of ventricular ectopy have been regarded as benign. The question that arises, however, is if there is a possibility that long-term endurance exercise per se could increase the risk for malignant ventricular arrhythmias and sudden death. This is a different question from the concern that a bout of exercise could trigger an event in an individual with cardiac disease. The question is whether long-term extreme endurance exercise could cause the development of a proarrhythmic ventricular substrate. There is now a suggestion in the literature that this indeed may be the case, albeit in rare circumstances. One hypothesis is based on the reports of elevated cardiac enzymes after prolonged endurance exercise such as marathons and the echocardiographic findings of acute right heart dysfunction, presumably from volume overload, immediately after the event. These changes resolve after 1 to 2 weeks, and have been considered benign. However, it is speculated that repeated episodes of right ventricular dysfunction might lead to the development of a cardiomyopathy.4 Indeed, some authors have coined the term “Phidippides cardiomyopathy.”12 You will recall that Phidippides was the Greek messenger who died suddenly, having delivered his victory message in Athens after running the 26.2 miles from Marathon in 490 BC. Phidippides cardiomyopathy is characterized by patchy fibrosis in the right ventricle and interventricular septum, documented by MRI.12 A rat model of extreme exercise demonstrated a similar pattern of fibrosis. Such areas of fibrosis could be a substrate for ventricular arrhythmias.13
Finally, the other mechanism by which extreme endurance exercise might create a substrate for malignant ventricular arrhythmias is paradoxically the progression of coronary artery disease. Although we know that moderate exercise reduces the risk of coronary artery disease, very recent observational studies suggest that extreme endurance exercise might be associated with higher coronary calcium scores and burden of atherosclerosis than expected.4 Why this paradoxical effect might occur has been hypothesized to be due to prolonged exercise causing endothelial damage, increased oxidative stress and inflammation, and thus counteracting the beneficial effects. The concept of a “U shaped” curve with regards to exercise has therefore arisen; inactivity carries elevated risk that is reduced by exercise up to a point, after which no further survival gain accrues and risk may increase.4,14 The point at which risk increases is not clear, but for instance, with regard to running, O’Keefe and Lavie suggest that there is no further survival benefit to be obtained from running more than 20 miles per week.14
Conclusions
Despite the foregoing concerns, any possible risks of prolonged endurance exercise must be put into perspective. So far, the data is largely observational, relatively new, and applicable to only a fraction of the population who participate in endurance exercise. As a public health issue, inactivity and lack of regular exercise should remain our major focus. Our priority as healthcare professionals must be to encourage regular, moderate exercise for its many benefits, and we should set an example in this regard. Moderate exercise such as brisk walking up to 30 minutes most days a week is enough to obtain most of the reported benefit from exercise. On the other hand, we should be aware and counsel the minority who are engaged in long-term, serious endurance exercise of some possible risks. I think we can say that high-volume endurance exercise carried on into middle and later life is associated with an increased risk of atrial fibrillation and possibly both benign and malignant ventricular arrhythmias. Having done this review, I now ponder whether I should run another marathon. I may consider the advice given by Hippocrates, a contemporary of Phidippides: ‘if we could give every individual the right amount of nourishment and exercise, not too little and not too much, we would have found the safest way to health.’
Disclosure: Dr. Gilligan has no conflicts of interest to report.
References
- Sagal P. He gave his all. The enduring legacy of a marathoner and a man. Runner’s World. November 2012:66-68.
- Kim JH, Malhotra R, Chiampas G, et al. Cardiac arrest during long-distance running races. N Engl J Med. 2012;
- 366(2):130-140.
- Thompson PD, Franklin BA, Balady GJ, et al. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115(17):2358-2368.
- O’Keefe JH, Patil HR, Lavie CJ, et al. Potential adverse cardiovascular effects from excessive endurance exercise. Mayo Clin Proc. 2012;87(6):587-595.
- Turagam MK, Velagapudi P, Kocheril AG. Atrial fibrillation in athletes. Am J Cardiol. 2012;109(2):296-302.
- Calvo N, Brugada J, Sitges M, Mont L. Atrial fibrillation and atrial flutter in athletes. Br J Sports Med. 2012;46 Suppl 1:i37-43.
- Koopman P, Nuyens D, Garweg C, et al. Efficacy of radiofrequency catheter ablation in athletes with atrial fibrillation. Europace. 2011;13(10):1386-1393.
- Calvo N, Mont L, Tamborero D, et al. Efficacy of circumferential pulmonary vein ablation of atrial fibrillation in endurance athletes. Europace. 2010;12(1):30-36.
- Baldesberger S, Bauersfeld U, Candinas R, et al. Sinus node disease and arrhythmias in the long-term follow-up of former professional cyclists. Eur Heart J. 2008;29(1):71-78.
- Heffernan KS. How healthy were the arteries of Phidippides? Clin Cardiol. 2012;
- 35(2):65-68.
- Biffi A, Maron BJ, Culasso F, et al. Patterns of ventricular tachyarrhythmias associated with training, deconditioning and retraining in elite athletes without cardiovascular abnormality. Am J Cardiol. 2011;107:697-703.
- Trivax JE, McCullough PA. Phidippides cardiomyopathy: a review and case illustration. Clin Cardiol. 2012;35(2):69-73.
- Benito B, Gay-Jordi G, Serrano-Mollar A, et al. Cardiac arrhythmogenic remodeling in a rat model of long-term intensive exercise training. Circulation. 2011;123(1):13-22.
- O’Keefe JH, Lavie CJ. Run for your life ... at a comfortable speed and not too far. Heart. 2012 Nov 29. [Epub ahead of print]

