

Developing a Robust Remote Monitoring Program in Your Practice: Clinical, Economic, and Workflow Considerations
 When implemented efficiently, remote monitoring for cardiac implantable electronic devices is a financially sound practice strategy. However, establishing an effective practice workflow to manage the panoply of new information has a number of challenges. In this article, we will briefly discuss the clinical and financial impact of remote monitoring, strategies for practice staffing and information management, as well as practice workflow.
When implemented efficiently, remote monitoring for cardiac implantable electronic devices is a financially sound practice strategy. However, establishing an effective practice workflow to manage the panoply of new information has a number of challenges. In this article, we will briefly discuss the clinical and financial impact of remote monitoring, strategies for practice staffing and information management, as well as practice workflow.
Introduction
The feasibility and safety of remote monitoring (RM) of cardiac implantable electronic devices (CIED) has been well established.1-5Clinicians can survey remotely monitored information for clinically actionable events, including arrhythmia burden and device therapies, as well as biometric parameters such as those used in heart failure management. In addition, RM provides a means to monitor lead integrity in an era where clinical recalls are problematic.
Reimbursement policy has begun to favor initiatives that minimize hospital admissions and repeated office visits. For example, the Remote Monitoring Access Act of 2007, an amended title XVIII of the Social Security Act, provides coverage for remote patient management services under Medicare. Another example of policy driving clinical practice is the Hospital Readmissions Reduction Program, whereby non-compliant care systems stand to suffer up to a 3% cut in Medicare DRGs.6 In essence, we must all demonstrate good outcomes with cost savings — that is, effectively do more with less. With efficient workflow processes in place, we believe RM will not only facilitate safe patient care, but can improve outcomes and augment your practice’s revenue stream.
Clinical Benefit for Remote Monitoring
Clinical information gleaned from RM of CIEDs can be divided into three broad categories: 1) system integrity; 2) arrhythmia detection and therapies; and 3) biometric parameters. Clinical benefits for RM have been demonstrated in each of the above categories and include early recognition of generator and lead issues,3,4,7 reduced time from clinical event to diagnosis and decision making,1,3 as well as early detection of atrial fibrillation (AT/AF)8,9 and impending congestive heart failure.10
The Lumos-T Safely Reduces Routine Office Device Follow-Up (TRUST) trial, in a prospective randomized fashion, compared the efficacy and safety of BIOTRONIK’s RM (using a mobile, wireless transmitter) in 1,450 dual chamber ICD recipients. The study demonstrated that home RM resulted in a significant, 45% reduction in the primary endpoint (scheduled and unscheduled office visits for device evaluation). The median time to detection and management of device and lead issues was significantly reduced. The time from an arrhythmic event to physician evaluation was reduced from a median of 36 days in the conventional monitoring arm to one day in the RM arm.4 Since device and lead malfunctions are potentially dangerous and may not be easily apparent to the patient from a clinical standpoint, early detection by home RM thus significantly improves patient safety.4
Similar results were shown in the multicenter, randomized Clinical Evaluation of Remote Notification to Reduce Time to Clinical Decision (CONNECT) trial. The study followed 1,197 patients over 15 months and showed that patients in the RM arm had a significant reduction in the mean time from an event to clinical decision making (4.6 days vs. 22.6 days in the conventional monitoring arm). RM was also associated with a reduced length of cardiovascular hospitalization.3 Medtronic has incorporated lead integrity alert algorithms into its CareLink RM system for early detection of Sprint Fidelis ICD lead failures. The system detects changes in lead integrity and provides an audible alert to the patient, warning of impending lead failure and inappropriate shocks.7 Similarly, BIOTRONIK’s ECOST trial demonstrated a reduced number of ICD therapies and subsequent improvement in battery life in patients randomized to RM versus those who were not.5
Another important instance in which RM trumps conventional monitoring is early detection of atrial and ventricular arrhythmias, which avoids delay in intervention. Particularly important is the detection and quantification of sub-clinical AT/AF. The ASSERT trial established that subclinical atrial tachyarrhythmias (atrial high rate episodes >190 bpm for >6 min) are associated with a 2.5 times higher risk of developing ischemic stroke or systemic embolism and a 5.5 times increased risk of future development of AF.8 The prospective, observational TRENDS study evaluated the relationship between atrial arrhythmia burden and thromboembolic risk in 2,486 patients with pacemakers and ICDs and a CHADS2 score ≥1. The study showed that a single AT/AF episode >5.5 hours in a 30-day period doubled the thromboembolic risk when compared to those with no AT/AF episodes.9 Researchers continue to pursue whether or not early AT/AF detection improves outcomes. The ongoing IMPACT trial plans to evaluate the hypothesis that early anticoagulation in patients with ICDs and CRT-Ds whose AT/AF was detected by RM will result in stroke reduction. This randomized, prospective study aims to establish the AT/AF threshold that warrants anticoagulation as well as define the clinical utility of home RM in CEIDs.11
For heart failure patients, clinically apparent changes such as weight change and dyspnea appear too late to prevent hospitalization. It makes sense that hospitalizations for heart failure can be reduced with early information such as percentage of biventricular pacing, measurement of thoracic impedance, heart rate variability, and activity level. Intrathoracic impedance monitoring has been shown to be a useful surrogate for pulmonary fluid status, allowing detection of heart failure progression before it becomes clinically apparent.10 Studies such as OptiLink-HF12 and IN-TIME13 are underway that that will provide us clear answers on whether early detection of congestion through RM improves hard clinical endpoints.
In summary, utilization of RM enables early identification of lead, device, as well as arrhythmia issues that translates into significant clinical benefits. Registry data have suggested a significant reduction in mortality in those ICD patients who undergo regular remote follow-up.2 Studies are ongoing that seek to quantify the benefit of RM on mortality, as well as for stroke prevention in AT/AF11 in a prospective, randomized fashion.
Economic Impact
Remote monitoring offers two potential economic benefits. The first relates to reimbursement for remote quarterly device checks, which are compensated at higher levels than in-office visits. Many organizations and device manufacturers have endeavored to quantify this revenue differential. Perhaps of greater importance is the possibility that RM can reduce healthcare expenditures. Several studies have pointed to lower spending due to RM and include results such as an 18% reduction in mean hospital stays,3 the reductions in office visits and physician hours,14 and a 41% reduction in the cost of routine ICD follow-up after a switch to RM.15 These savings are becoming increasingly important as reimbursement shifts from fee-for-service models to global or capitated financial arrangements. Studies are currently under way that will further examine the cost-effectiveness of RM.16,17
Practice Workflow
RM requires deliberate planning, and practices that deploy intentional approaches succeed far more than those that have unplanned or unstructured RM workflows. The approach needs to be intentional for all stakeholders including patients, many of whom who still equate RM with transtelephonic monitoring of old, and feel that it may take too much work on their behalf.1,18 New capabilities such as radiofrequency-enabled devices have allowed greater capabilities but require buy-in from physicians, staff, patients, and family.
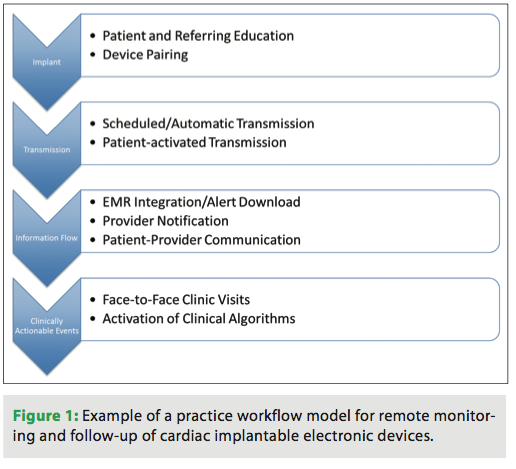
The practice workflow begins prior to device implantation at the pre-procedural visit. At this time, office staff should educate the patient about the benefits and logistics of remote monitoring. Immediately after implant and prior to discharge from the hospital, revisiting RM with the patient and ideally pairing the device with the RM station helps to reinforce the importance of the process and improves compliance.19 Contacting the patient to walk them through the hook-up and first transmission is valuable. The earlier they become comfortable with the technology, the greater the compliance will be. Those patients without landline phones may have a cell phone option, depending on the vendor. This is likely a trend the industry has started to and will need to embrace and support given the number of families abandoning landlines. Finally, a system should be put in place to encourage regular remote transmissions, particularly in patients living with a device under recall. An example of a ‘real-world’ practice workflow for RM is shown in Figure 1.
Adoption of a remote monitoring program comes with a number of challenges, including a change in the patient-provider dynamic as the patient “sees” the physician less. Many patients are reluctant to adopt new technologies and worry that fewer encounters may translate to poor care. On the contrary, more remote “touches” may actually result in better outcomes because providers will scrutinize patient data more often.2,5 Another challenge lies in the efficient retrieval and funneling of relevant clinical information to providers and establishment of a mechanism for clinical action that preserves productivity. Clinical algorithms for commonly encountered clinical scenarios, such as incidental AT/AF, impedance changes, or noise on a previously recalled ICD lead, should be developed. Careful delineation of responsibility for information download and triage is critical. At the same time, as much as possible, non-clinical personnel should carry out data transfer. Once clinical parameters have been established, support staff can download information, contact patients for follow-up, and facilitate integration of the information into the EMR. Data integration methodologies vary, with some requiring manual intervention, and others aiming for complete “hands-free integration.”
Practice Workflow Models
With over a decade of field experience with RM, practices have deployed several models for managing the workflow of patients. Some have internalized the work using a full complement of practice resources (staff and technology) and others have deployed middleware (agnostic and proprietary). Regardless of structure, the goal is to optimize efficiency and improve patient care (Figure 1). Each has its own merits depending on practice size (i.e., electrophysiologist [EP] alone, cardiologists and EP in a joint practice), volume of implants, and level of RM adoption. The following real-life practices highlight two strategies that have led to RM success.
Model #1: In-House
AMS Cardiology, located in Abington, Pennsylvania, deploys its own resources to run its RM program in which it monitors several thousand patients. AMS has 18 cardiologists, 3.5 full-time equivalent EPs and 3 device nurses. The practice performed an RM compliance analysis and discovered that out of approximately 10,000 possible remote checks, they were only capturing 16%. As one of their EPs, Dr. Richard P. Borge, Jr., noted, “This had possible negative implications for patient care and we were losing money. We had to examine a new strategy for active patient management.” Active management, meaning that the practice would take an intentional approach to staffing, management, and oversight of RM, required a departure from the “honor system” for both patients and staff. The days of hoping that the transmission would occur gave way to a much more structured approach. However, active management, if done properly, would also mean a large influx of work as compliance improved. Having ramped up the success of their RM practice, the staff noted the following success factors:
- Identify and train staff or staff members that focus on remote monitoring. Expecting anyone and everyone to engage in RM, without clearly defined roles, is suboptimal. The “master of all trades, jack of none mentality” limits efficiency.
- Select appropriate patients. Not all are good candidates from a compliance and health perspective. Educating the patient and the patient’s family improves compliance.
- Optimize administrative functions. AMS bills quarterly instead of daily for all RM patients. Cash flow and policy must allow for such a procedural change, but AMS has minimized daily churn related to RM billing. Hence, AMS accumulates its RM billing and completes it on the last few days each quarter for patients that qualify for RM. By processing all RM codes at the same time, AMS has experienced billing efficiency improvements. Also, platforms such as BIOTRONIK provide alerts (with the practice protocol dictating the timeframes) to practitioners if no RM transmissions occur, thus helping to ensure patient compliance.
In yet another model, FryeCare Heart Diagnostics in Hickory, NC, a clinic with ~3,800 device patients (roughly 60% remote), and one device clinician, schedules two virtual clinic days to manage remote patients. On Mondays and Fridays, device staff schedule remote patients every 15 minutes, treating printed reports like a virtual clinic visit. On “non-virtual device days,” practice staff members allot an hour prior to the clinic’s opening to address any alerts or patient needs requiring a clinician. This model has led to an increase in the administration of the program and client adherence, and the practice has experienced a greater increase in revenue and profit.
Model #2: Outsourced
Dr. Suneet Mittal, Director of Electrophysiology at The Valley Hospital Health System, wrestled with some of the same challenges that AMS Cardiology experienced. As the number of encounters began to increase, they were not enrolling reliably. When they did enroll, transmissions did not regularly occur. When data were transmitted, it was not done on a regular, quarterly basis. Dr. Mittal noted “this was a national problem as data from Medtronic, via CareLink, demonstrated that only two-thirds of patients were enrolled into a remote monitoring program and, of these patients, only 5% had quarterly data transmissions. Additionally, our nurse practitioner (NP), whom we hired for device follow-up, became more or less a technician, with 30% of her time focused on administrative tasks. Her ability to carry out patient care was becoming limited.” After careful analysis, the practice moved to an insourced solution with ScottCare Cardiovascular Soltions/Ambucor Health Solutions. In this model, the practice submits the enrollment form while the company ensures that the patient transmits data, addresses any transmission delays, completes reports, notifies physicians of any alerts, and generates of list of patients to those on Dr. Mittal’s staff who handle the charges.
Conclusions
With clinical trials demonstrating the clinical and financial benefits of RM, the question of “if” or “why” one should deploy RM is being transitioned to “how.”20 The question of “how” is even more important today as the days of industry representatives serving as “off balance-sheet labor” for practices will fast become an unsustainable model (for both device companies and practices). Additionally, the sheer prevalence of cardiovascular disease, which consumes almost 20% of health spending, and other conditions like AT/AF (expected to grow from an estimated 2.66 million in 2010 to 12 million in 205021) will drive utilization of care to new heights. The increased utilization does not even account for new clinical applications of RM such as direct left atrial pressure monitoring (LAPTOP-HF trial), remote device programming, and advanced use of RM for anticoagulation therapy.11 It is clear that RM is the way of the future and with the right planning, practices can deploy a workflow strategy that facilitates better patient care while allowing optimization of scarce practice resources.
Disclosures: Dr. Sutton and Mr. D’Orazio report they are employees of Sage Growth Partners, LLC, a health strategy firm with relationships to St. Jude Medical and BIOTRONIK. Dr. Gopinathannair reports that outside this submitted work, he is a consultant for St. Jude Medical and has received honoraria from Boston Scientific.
References
- Crossley GH, Chen J, Choucair W, et al. Clinical benefits of remote versus transtelephonic monitoring of implanted pacemakers. J Am Coll Cardiol. 2009;54(22):2012-2019.
- Saxon LA, Hayes DL, Gilliam FR, et al. Long-term outcome after ICD and CRT implantation and influence of remote device follow-up: the ALTITUDE survival study. Circulation. 2010;122(23):2359-2367.
- Crossley GH, Boyle A, Vitense H, et al. The CONNECT (Clinical Evaluation of Remote Notification to Reduce Time to Clinical Decision) trial: the value of wireless remote monitoring with automatic clinician alerts. J Am Coll Cardiol. 2011;57(10):1181-1189.
- Varma N, Epstein AE, Irimpen A, et al. Efficacy and safety of automatic remote monitoring for implantable cardioverter-defibrillator follow-up: the Lumos-T Safely Reduces Routine Office Device Follow-up (TRUST) trial. Circulation. 2010;122(4):325-332.
- Guedon-Moreau L, Lacroix D, Sadoul N, et al. A randomized study of remote follow-up of implantable cardioverter defibrillators: safety and efficacy report of the ECOST trial. Eur Heart J. 2012 Dec 13.
- “Readmissions Reduction Program.” CMS.gov. 1 Aug. 2012. Web. 19 Jan. 2013. <https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html)>.
- Swerdlow CD, Gunderson BD, Ousdigian KT, et al. Downloadable algorithm to reduce inappropriate shocks caused by fractures of implantable cardioverter-defibrillator leads. Circulation. 2008;118(21):2122-2129.
- Healey JS, Connolly SJ, Gold MR, et al. Subclinical atrial fibrillation and the risk of stroke. N Engl J Med. 2012;366(2):120-129.
- Glotzer TV, Daoud EG, Wyse DG, et al. The relationship between daily atrial tachyarrhythmia burden from implantable device diagnostics and stroke risk: the TRENDS study. Circ Arrhythm Electrophysiol. 2009;2(5):474-480.
- Tang WH, Tong W. Measuring impedance in congestive heart failure: current options and clinical applications. Am Heart J. 2009;157(3):402-411.
- Ip J, Waldo AL, Lip GY, et al. Multicenter randomized study of anticoagulation guided by remote rhythm monitoring in patients with implantable cardioverter-defibrillator and CRT-D devices: Rationale, design, and clinical characteristics of the initially enrolled cohort The IMPACT study. Am Heart J. 2009;158(3):364-370 e1.
- Brachmann J, Bohm M, Rybak K, et al. Fluid status monitoring with a wireless network to reduce cardiovascular-related hospitalizations and mortality in heart failure: rationale and design of the OptiLink HF Study (Optimization of Heart Failure Management using OptiVol Fluid Status Monitoring and CareLink). Eur J Heart Fail. 2011;13(7):796-804.
- Arya A, Block M, Kautzner J, et al. Influence of home monitoring on the clinical status of heart failure patients: design and rationale of the IN-TIME study. Eur J Heart Fail. 2008;10(11):1143-1148.
- Elsner CH, Piorkowski C, Taborsky M, et al. A prospective multicenter comparison trial of home monitoring against regular follow-up in MADIT II patients: additional visits and cost impact. Comput Cardiol. 2006;33:241-244.
- Raatikainen MJ, Uusimaa P, van Ginneken MM, et al. Remote monitoring of implantable cardioverter defibrillator patients: a safe, time-saving, and cost-effective means for follow-up. Europace. 2008;10(10):1145-1151.
- Marzegalli M, Landolina M, Lunati M, et al. Design of the evolution of management strategies of heart failure patients with implantable defibrillators (EVOLVO) study to assess the ability of remote monitoring to treat and triage patients more effectively. Trials. 2009;10:42.
- Ricci RP, D’Onofrio A, Padeletti L, et al. Rationale and design of the health economics evaluation registry for remote follow-up: TARIFF. Europace. 2012;14(11):1661-1665.
- Schoenfeld MH. Transtelephonic versus remote monitoring of cardiovascular implantable electronic devices: is one approach to be preferred? J Am Coll Cardiol. 2009;54(22):2020-2022.
- Apostolakos C, Ren C. Patient Adherence in Remote Follow-up of Cardiovascular Implantable Devices. Cardiovascular Medicine and Surgery (COAST) Conference; 2011.
- McDaniel D, DeMarco C, D’Orazio D. Remote Monitoring for Cardiac Arrhythmia: Its Legacy and Growing Importance in Advancing Clinical and Economic Outcomes. A Sage Growth Partners White Paper. September 2012. <https://www.sage-growth.com/wp-content/uploads/2011/11/Biotronik_Remote_Monitoring_WP11.pdf>.
- “Atrial Fibrillation Fact Sheet.” Centers for Disease Control and Prevention. 20 Dec. 2010. Web. 19 Jan. 2013. <https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_atrial_fibrillation.htm)>. 2010.

