

Common Questions About Robotic Magnetic Navigation
 Dr. Ramaswamy is an expert on the Stereotaxis Magnetic Navigation system and was among the first to demonstrate its advantages in reducing radiation exposure. In collaboration with Dr. Carlo Pappone, he performed the first bidirectional live case demonstration of the technology. For this article, EP Lab Digest asked Dr. Ramaswamy to answer common questions about robotic magnetic catheter navigation (RMN).
Dr. Ramaswamy is an expert on the Stereotaxis Magnetic Navigation system and was among the first to demonstrate its advantages in reducing radiation exposure. In collaboration with Dr. Carlo Pappone, he performed the first bidirectional live case demonstration of the technology. For this article, EP Lab Digest asked Dr. Ramaswamy to answer common questions about robotic magnetic catheter navigation (RMN).
 Since the introduction of RMN, the technology has been adopted by many centers around the world, but has not become a ubiquitous presence in every lab. Most EP professionals have a basic awareness of robotic technologies, but often have questions about its role and uses. RMN involves navigation of a flexible, magnet-tipped ablation catheter within the cardiac chambers by variation of a magnetic field using computerized control of external, rotating permanent magnets at the patient’s bedside.
Since the introduction of RMN, the technology has been adopted by many centers around the world, but has not become a ubiquitous presence in every lab. Most EP professionals have a basic awareness of robotic technologies, but often have questions about its role and uses. RMN involves navigation of a flexible, magnet-tipped ablation catheter within the cardiac chambers by variation of a magnetic field using computerized control of external, rotating permanent magnets at the patient’s bedside.
What are the advantages of RMN over traditional, manual catheter navigation?
Two benefits have been demonstrated through clinical trials and inherent characteristics of the system. First, radiation exposure to the patient and the lab staff is significantly reduced. Second, there is a decreased risk of cardiac perforation due to the flexibility of the catheter. Other advantages include the ability to navigate difficult anatomy such as in complex congenital heart disease, and catheter stability at some sites (even with normal anatomy) may be improved with the magnetic catheter. Mapping is more detailed and precise, as stable and consistent contact can be achieved without the need for excessive force. For complex arrhythmias, such as in non-isthmus-dependent, macroreentrant atrial tachycardias or reentrant ventricular tachycardia, a high-density and accurate map is often the best means to achieve success with ablation. Finally, robotic control of the catheter places the electrophysiologist in a “cockpit” environment in the control room, enabling the direct involvement in construction and annotation of the 3D electroanatomic map, interpretation of entrainment data and electrograms, and observation of AV conduction and response to ablation. RMN allows the electrophysiologist to concentrate on mapping and ablation, rather than the manual task of catheter manipulation.
What are the disadvantages of RMN?
Low contact force, though an advantage in virtually eliminating perforation risk as described above, can limit RF lesion size. This can be a cause of ablation failure in certain situations where greater lesion depth is required, such as in the cavotricuspid isthmus.1 There are other situations where manual catheters may be better. In cases of left-sided accessory bypass tracts in a small left atrium, it can be difficult to advance the catheter such that all catheter magnets are in the left atrium, and freedom of movement can be limited, particularly to create a loop of the shaft. Instability on the annulus, or decreased contact force, or both, can result. In such circumstances, stiffness of the catheter shaft and tip promotes stability and contact. Another disadvantage of RMN is that manipulation of other hardware (such as a circular mapping catheter, guiding sheath, or intracardiac echo) may require leaving the control room many times during a procedure, diminishing the benefit of “remote” control. (This problem has been solved with the development of a robotic controller for non-ablation catheters for use with RMN; it has been demonstrated to be safe and reliable in Europe, but remains unavailable in the U.S.)
Is RMN faster?
In the only prospective, randomized comparison of manual vs. magnetic catheter ablation for SVT,2 there was no difference in procedural time. A learning curve has been well-described in other studies, with similar procedural times afterwards generally being the case. Some reports have described longer procedural times for ablation for AF with RMN3 and atrial flutter.1 In my experience and from observations of other skilled RMN labs, I have noted that RMN neither slows nor accelerates the completion of the procedure, and the primary determinants of procedure time have been local habits and protocols for mapping/ablation. The recently introduced, next-generation RMN system by Stereotaxis (Epoch) produces faster catheter movements and improvements in automatic functionality. Whether these improvements will translate to shorter procedure time will be determined in future reports (hopefully from direct comparisons to manual).
Can RMN be used with EnSite NavX?
There is direct integration of Biosense Webster’s Carto system with the RMN software, but many labs use St. Jude Medical’s NavX system with RMN.
Can patients with cardiac implanted devices undergo RMN?
The literature establishing safety with this patient population is growing, and it is common for patients with such devices to be brought to the RMN lab. It should be anticipated that the magnet-mode on the device will be activated (asynchronous pacing), but in general, temporary programming changes can be made so as to avoid interference with the EP study. I recommend interrogation of the device pre- and post-procedure.
Are special techniques used with RMN?
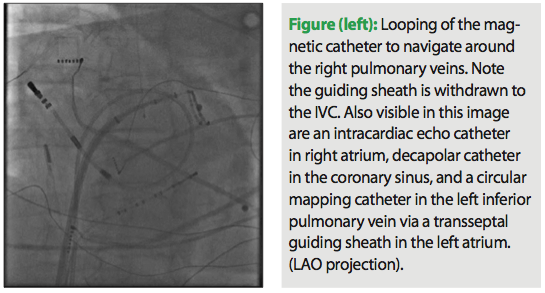
Operators quickly become accustomed to maneuvering the catheter using vector navigation and without tactile feedback. One notable difference with manual catheter manipulation is the sheath location often used with the RMN catheter. Most commonly, a minimally curved sheath tip (e.g., SL0) is used. For left atrial procedures, I keep the sheath tip in the IVC to maximize and allow for full magnet exposure and unrestricted movement of the flexible catheter shaft. This enhances the ability to reach all areas of the chamber. On the other hand, sheath support can be helpful for slow pathway ablation, and the sheath is advanced as much as possible while still maintaining exposure of all three magnets with the tip at the target site. For access to the right pulmonary veins, a looping maneuver is commonly used (Figure 1), and this technique can also be helpful for mapping the annulus. For LV mapping, a transseptal approach and Mullins-type sheath is frequently preferable to a retrograde aortic approach. In all cases, the adequacy of tissue contact should be assessed by integrating information from fluoroscopic observations, RMN software contact data, the 3D electroanatomic map and catheter icon, and electrogram morphology. n
Disclosure: Dr. Ramaswamy has no conflicts of interest to report.
References
1. Vollmann D, Lüthje L, Seegers J, et al. Remote magnetic catheter navigation for cavotricuspid isthmus ablation in patients with common-type atrial flutter. Circ Arrhythm Electrophysiol. 2009;2:603-610.
2. Wood M, Orlov M, Ramaswamy K, et al, Stereotaxis Heart Study Investigators. Remote magnetic versus manual catheter navigation for ablation of supraventricular tachycardias: a randomized, multicenter trial. Pacing Clin Electrophysiol. 2008;31(10):1313-1321.
3. Miyazaki S, Shah AJ, Xhaët O, et al. Remote magnetic navigation with irrigated tip catheter for ablation of paroxysmal atrial fibrillation. Circ Arrhythm Electrophysiol. 2010;3(6):585-589.

