

Assessing Lifetime Value (LTV) of Patients: Lessons from a Dairy Farmer
I grew up working on a small dairy farm in Philadelphia, New York. I earned two dollars per hour bailing hay, milking cows, and doing chores. Aside from my wage, the cost of running that farm steadily rose, while other farms consolidated and drove down the price of milk. Like most, the small family farm I worked on did not survive.
“Collins Knoll Farm” in Chadwicks, New York, is different.
My Uncle Ed has been successfully running Collins Knoll Farm since Grandpa retired. He does everything possible to maximize the lifetime value (LTV) of every cow. LTV is a calculation that yields how much something is worth over a set time: like 5 years for a cow or 20 years for a patient. I’ll walk you through how Uncle Ed explained the LTV of a cow on his farm. I’ll then walk you through the LTV of a few patients.
Cow LTV Calculation
For the first two years of a cow’s life, Ed grows it and keeps it healthy. Then he has the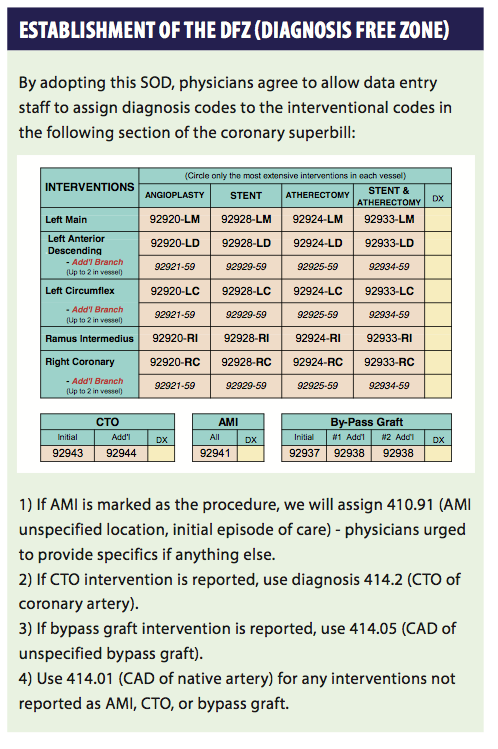 veterinarian come out to the farm to artificially inseminate it. If everything goes right, nine months later the cow gives birth and her milk comes in — Ed then milks her for just over 300 days. During the 300 days of milking, Ed does everything possible to make the cow comfortable and productive. Cows can eat as much as they want, they have regular checkups, and they are cooled in the summer and kept warm in the winter.
veterinarian come out to the farm to artificially inseminate it. If everything goes right, nine months later the cow gives birth and her milk comes in — Ed then milks her for just over 300 days. During the 300 days of milking, Ed does everything possible to make the cow comfortable and productive. Cows can eat as much as they want, they have regular checkups, and they are cooled in the summer and kept warm in the winter.
Because of all this tender loving care, a cow on Ed’s farm produces 29,000 pounds of milk each year — 7,000 pounds more than the New York state average. That really adds up when you consider that Ed is milking 760 cows!
Cows go through three breeding/milking cycles before they leave the farm for what Ed calls a “career change.” Each cow generates $8,685 in profit during the five years they are on the farm. When they leave, Ed gets about $1,000/cow from the meat packer. But the true value of each cow is much more than the sum of $9,685. You must also consider the value of the three calves the cow had during her milk-producing years. Each of the female calves will generate $9,685 in profit. If all of these three calves are female, the lifetime value of the cow mushrooms to $38,740. If we add in just one more generation of female calves, the lifetime value of the cow climbs to $125,905.
Of course, this estimate is inflated because it assumes that each calf is a girl. In reality, some of the calves will be male (bulls). A male calf does not add the same amount to our LTV calculation as a female calf. It is very easy to calculate the financial contribution of a male calf on the farm, and I bet you’ll be surprised at how low the number is.
“Big Ed’ was the last bull that lived on Collins Knoll Farm. Big Ed was on the farm to get cows pregnant. When he was successful, the farm avoided the cost of having the vet come out to artificially inseminate the cow, which costs $46. To calculate Big Ed’s LTV, we’d need to factor in how many cows he successfully got pregnant over a five-year reference term. So let’s say he got 100 cows pregnant every year for five years. Factoring in the $46, this represents $4,600 saved each year, which is $23,000 over the course of five years. We’d have to add in the $1,000 from the meat packer and then reduce the total revenue by the costs associated with having Big Ed on the farm to come up with his true LTV for five years. Since he required separate barn space, Big Ed was far more expensive to maintain than the average cow.
The Collins Knoll Farm has a different way to calculate LTV than the preceding calculation. Within a few weeks of birth, all bulls are sold at auction for about $100. That is the LTV of a bull.
There are a lot of parallels between dairy farming and operating a cardiology program. Successful cardiology programs consider the LTV of each patient category and go to extraordinary lengths to enhance the LTV of the most productive patients. In cardiology, the highest producing “cow” is the heart failure patient. The highest maintenance “bull” is the warfarin patient.
Heart Failure Patient LTV Calculation
An initial consult is performed for a new heart failure patient. If the doctor understands how to document and code for this visit, it will be a level five service (99205), which yields a national unadjusted Medicare reimbursement amount of $203.80.
Next, we implant a biventricular defibrillator in the patient. This yields $1,526.95. Code 33249-Q0 (ICD system implant) pays $909.09, code 33225 (left ventricular lead implant) pays $456.25, and the defibrillation threshold test code, 93641-26, pays $161.61 (50% of the $323.22 national allowed amount because the multiple procedure reduction applies).
One defibrillator programming evaluation (93284-26) is performed on the day of discharge ($60.22), and a second (93284) is performed at the time of the incisional site check. Since we can bill for the global service (i.e. we don’t attach the 26 modifier to code 93284), this device check pays $87.78.
A follow-up office visit should be provided and billed within the 90-day post-op period. For this visit, the doctor should report code 99214-24 and will receive $106.83. The 24 modifier is needed to convey that you are seeing the patient for management of an underlying condition rather than routine surgical recovery.
After the 90-day post-op period expires, we start seeing heart failure patients four times a year for office visits at $108.83 per visit. During two of these visits we conduct device programming evaluations (93284), which yield $87.78 each. We do remote monitoring of the device, which is billed four times a year with codes 93295 ($64.30) and 93296 ($26.20). We also report remote physiologic monitoring 12 times each year with codes 93297 ($25.52) and 93299 (approximately $30).
Excluding all the other services these patients will require, we will realize $3,616.70 for the initial implant and first year of follow-up care. Each subsequent year of patient management will yield $1,631.12 in professional service compensation. If the patient stays with our program for 20 years, they will yield $34,607.98 in professional service compensation.
Warfarin Patient LTV Calculation
Office visits are required twice a year (99214 – $106.83). INR testing is required monthly (85610 – about $5.40). While other services may be needed, these are the only routine services. All in, these patients bring in $278.46 each year. Like bulls on the farm, warfarin patients are very high maintenance — the administrative burden associated with scheduling and facilitating the 12 INR checks alone frequently depletes the entire annual yield. You also have to dedicate valuable space for your warfarin clinic, and doctors are exposed to increased liability — warfarin is one of the most common drugs involved in malpractice lawsuits. In short, over the same 20-year period, this patient will yield $5,569.20 in professional service compensation.
Increasing to Line Revenue
Like Uncle Ed, CardiologyBiller.Com goes to extraordinary lengths to maximize the LTV of our billing clients. Since we charge a small percentage of gross revenue, our compensation is aligned with client compensation — the better we do our job, the more everybody gets. We employ hundreds of proprietary tools, protocols, and initiatives that collectively help secure more compensation for clients than most billing companies ever could. I’ll share a few examples below.
Procedural Superbills
The superbill we use for electrophysiology, pacemaker, and defibrillator surgeries was published in the January 2014 edition of EP Lab Digest®. After training doctors on how to complete the form, we facilitate real-time, accurate coding of all EP and CRM procedures. We have a similar form for coronary procedures that has not been made public. However, I’m providing an excerpt of the coronary intervention section of the form and a corresponding Standard Operating Directive.
Before launching the superbill at a practice, we enter a written agreement with each physician that outlines exactly how diagnosis codes will be assigned to coronary interventions in the absence of a diagnosis being checked off on the form. For example, if the doctor checks off that he performed an acute myocardial infarction intervention, we will automatically assign a specific acute MI diagnosis code. If the doctor wants to report something else, he just checks off the appropriate diagnosis and it overrides the Directive.
This policy and superbill take a little bit of stress off of the doctors. This makes them a little more comfortable as well as more productive. It also eliminates a fair amount of administrative burden and some of the most common requests to physicians from the business office.
Hospital Charge Capture App
Another good example is our hospital charge capture application for iPhone and Android devices. Think about how you currently capture charges for hospital rounds and admissions. Perhaps your doctors have a printed schedule that they follow — hopefully they add on all new patients that get referred throughout the day. When that happens, they need to legibly write down the patient name, ID number, date of birth, date of admission, etc. Mistakes happen, consults go unbilled, and there is the potential for negative communication from the business office to the doctors, which can be stressful.
The hospital charge capture app improves this process, eliminates the stress, and effectively creates thousands of FTE physicians in the United States — 22 minutes per user, per day. That is how much time our app can save the average physician each day.
The app launches March 30 in Booth #707 at ACC.14 in Washington, DC. Here is how the app will work:
- The doctor takes a picture of his schedule for the day.
- That picture is routed to our U.S.-based data entry staff for processing.
- Within minutes, each patient from the schedule shows up in a bubble on the app.
- Click on the bubble to indicate the patient you are seeing, select the level of service and diagnosis, and you are done. On to the next bubble!
- If you get a new consult, just click “add patient” and your phone instantly turns into a high-speed camera. You can take three or four pictures of all the demographic paperwork — that is all anyone should need for billing.
Now picture your billing staff sitting in front of two monitors. One has your existing billing system up and functioning. The other has the live feed from each of your registered devices. Every picture is available to view and is in a legible format. In addition to helping save time and money, this app also helps doctors be more productive.
The Universal Programmer
The last big opportunity I’ll share with you is the one I’m most passionate about. MADIT-RIT demands sweeping change in device clinic protocol. I’m working on a solution that will facilitate and verify appropriate program settings for over 90% of all implanted pacemakers and defibrillators. If it works out like my friends are telling me it could, we will be able to offer what I am temporarily calling “The Universal Programmer” to the world, for free. The launch date is set to take place on March 29 in Booth #707 at ACC.14.

