

ADVERTISEMENT
ANESTHETIC: A Novel System to Teach, Promote and Enhance Patient-Centered Communication
Effective patient-centered communication is critical in conveying important information between the health care provider and the patient. In the era of electronic medical records, with all the documentation requirements, it may be easy to forget the key components necessary to provide excellent patient-centered communication. The “ANESTHETIC” mnemonic (Figure 1) was developed by an anesthesiologist who works closely with the electrophysiology section at Winthrop University Hospital. The mnemonic provides a rapid reinforcement tool of the validated key elements in order to optimize doctor-patient communication. This paper describes the tool in a discussion between its developer and an early adapter.
INTRODUCTION FROM DR. COHEN
As a practicing electrophysiologist, cardiologist, and clinician, I am always looking for ways to improve on my clinical performance. I was intrigued by hearing about a method developed by one of my colleagues, Dr. Matthew Giuca. Dr. Giuca, one of the anesthesiology attendings at Winthrop University Hospital, has an interest in teaching the medical students and is committed to improving his quality performance as a physician. Similarly, I share many of the same interests and goals with Dr. Giuca, and seek a similar improvement in my own practice. Anesthesiology and electrophysiology are partners in taking care of many of our patients in the electrophysiology arena. They often require more than just conscious sedation (i.e., deep sedation), and working with anesthesiology has been very beneficial to the care of the patients at Winthrop University Hospital. In the following section, Dr. Giuca will present the context and theory of his simple mnemonic called ANESTHETIC, which describes a process that can enhance patient-centered communication. He will describe the rationale behind the anesthetic mnemonic and the literature on which it is based. He will also explain a way an observer could score the successful utilization of the key performance areas indicated by the mnemonic when interacting with patients. In addition, he will describe how adapting this communication style has a positive effect on students as well as patients.
CONTEXT AND THEORY: DR. GIUCA
“Medicine is an art whose magic and creative ability have long been recognized as residing in the interpersonal aspects of the patient-physician relationship.”1
Effective communication is the most essential aspect of patient care. It is an ACGME core competency, and a component of every skill necessary for successful treatment of our patients.2,3 Competence in medicine as defined by Epstein et al is “the habitual and judicious use of communication, knowledge, technical skills, clinical reasoning, emotions, values and reflection in daily practice for the benefit of the individuals and communities being served.”4 A doctor’s communication and interpersonal skills encompass the ability to gather information in order to facilitate accurate diagnosis, counsel appropriately, give therapeutic instructions, and establish caring relationships with patients.
Patients consistently state that physicians need to improve their communication skills. Moreover, patients rate elements representing information and communication highest in importance when surveyed about their expectations.5,6 Compounding this problem is that physicians underestimate the need for improvement in these skills and overestimate their own proficiency.7-10 To participate in the resolution of this problem, I studied peer-reviewed articles pertaining to the communication requests of patients. With this information, the ANESTHETIC mnemonic teaching tool was devised to teach and facilitate efficient patient-centered communication.11,12
The principles of patient-centered medicine date back to the ancient Greek school of Cos. However, patient-centered medicine has not always been common practice. For example, during the 1950s to the 1970s, most doctors considered it inhumane and detrimental to patients to disclose bad news.11,13-15
Collaboration and the discussion of options is the most desired communication model. Patients view themselves as health consumers and they desire shared decision making. This is the keystone and central premise of patient-centered communication.16-18 Employing patient-centered communication attributes has been shown to increase patient satisfaction and compliance as well as decrease pain and litigation, while improving outcomes.2,19-23 The curriculum designed around use of the ANESTHETIC mnemonic tool will hopefully improve the interactions between patients and providers. I believe this tool will be useful in educating students and their mentors for the benefit of our patients.
OBJECTIVES
For patients
- Increased patient-centered communication
- Create a partnership with clinicians and share control of their healthcare
- Obtain better medical outcomes and satisfaction
For physicians
- Improve patient outcomes and satisfaction
- Reinforce awareness of patients’ desire for information and collaboration
- Strengthen partnership with patients
- Improve communication abilities
For students
- Augment training of medical students and health professionals
- Prepare future physicians for the increasing focus on patient-centered care
- Teach students an efficient patient-centered communication style
METHODOLOGY
The acronym “ANESTHETIC”, which corresponds to the actions and attributes that patients state they would like exhibited by their caregivers, was utilized by Dr. Cohen. His use and adoption of the mnemonic represents an important step in improving communication between patients and physicians. Attending involvement in improving patient-centered communication directly addresses the needs of our patients while evoking one of the most powerful teaching tools: modeling. Teaching by positive modeling of good communication actually contributes to better patient outcomes and education.24 This well-studied concept is intuitive. If Dr. Cohen exhibits these actions and attributes while caring for his patients, then medical students, residents, fellows and physician assistants will undoubtedly mimic the behavior. Our first step was to observe Dr. Cohen and score his interactions and inherent adherence to the actions and attributes contained in our mnemonic. We scored Dr. Cohen using a Likert scale designed specifically for the ANESTHETIC tool. After observing Dr. Cohen with patients, we trained him on the use of the ANESTHETIC tool. We then discussed where we saw opportunities for integration. Dr. Cohen learned quickly and subsequent observations displayed complete adherence to the ANESTHETIC technique. The following is a detailed outline of the acronym itself:
“ANESTHETIC” is a 10-letter acronym which represents ten important steps for a clinician to remember during any patient encounter. Each letter, which stands for a specific step, is a set of desirable behaviors expected from the physician towards a patient:16,28-37
stands for a specific step, is a set of desirable behaviors expected from the physician towards a patient:16,28-37
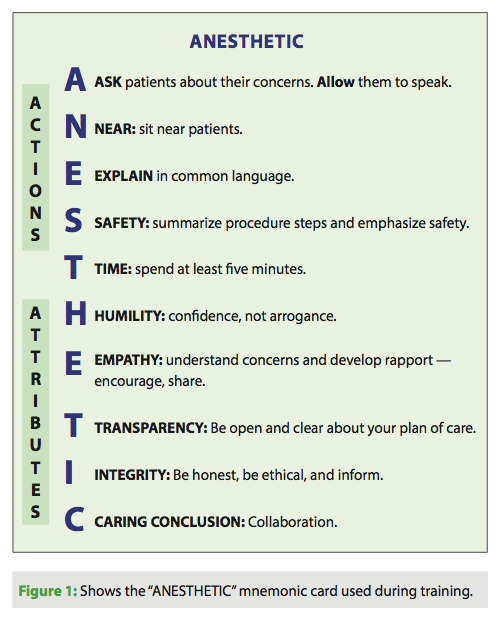
A: Ask the patient what they would like to learn about their anesthetic and allow them to speak more than you.
N: Near — always sit next to the patient so they can see you clearly (positive body language is important) and speech can be at a comfortable volume.
E: Explain in common language — avoid jargon as it confuses the patients and creates a barrier to understanding.
S: Safety — you are concerned about their safety; give them an example of how you will protect them (i.e., “I will pad your elbows to protect your arms from nerve injury”).
T: Time — goal of five minutes or more.
H: Humility — display it at all times — arrogance will destroy rapport. Confidence is always perceived well. Be aware of the difference.
E: Encourage the patient to speak about their concerns. Earn trust and rapport — share something about who you are as a person.
T: Transparency — Tell them about your concerns and plans to care for them, including discussions you had with the surgeon if appropriate.
I: Inform them of anesthetic options if there are any. Your recommendations will be welcomed, but the patient will participate in the decision.
C: Caring Conclusion — review discussion and Confirm with patient that all questions were answered and they feel Comfortable proceeding.
LIKERT SCALE
The ANESTHETIC mnemonic process includes a scoring sheet. The scoring methodology is similar to the standard Likert scale. “A Likert scale is a psychometric scale commonly involved in research that employs questionnaires. It is the most widely used approach to scaling responses in survey research, such that the term is often used interchangeably with rating scale, or more accurately the Likert-type scale, even though the two are not synonymous. The scale is named after the psychologist Rensis Likert.38
The following is an example of the Likert scale used in the simulation exercise:
Nonverbal communication
0) Stands more than five feet from the patient, makes dismissive gestures or focuses on note taking more than patient eye contact
1) Stands near the patient, initiates eye contact
2) Stands near the patient, initiates eye contact, initiates appropriate touch (i.e., handshake)
3) Sits near patient, makes eye contact, initiates appropriate touch
4) Sits near patient, makes eye contact, initiates appropriate touch and does not interrupt the patient
Verbal communication
0) Uses substantial jargon, offered no examples of safety measures, failed to elucidate patient’s concerns, failed to offer alternatives and no conclusion or summary are offered
1) Discussed safety measures and procedure but failed to elucidate patient concerns or offer alternatives
2) Addressed patient concerns, use of safety measures and alternatives but used substantial jargon
3) Addressed patient concerns, use of safety measures and alternatives and explained clearly and understandably
4) Asks the patient what they would like to know, gives an example of a safety measure, explains in common language, discusses concerns and alternatives, offers a conclusion to the interview
Receptivity
0.) Is critical of or demeaning of patient’s questions or rushes patient’s questions
1.) Never asks the patient if they have a question but answers questions when the patient brings them up
2.) Asked the patient if they have questions
3.) Asked the patient if they understood and if they had questions
4.) Asked the patient what they wanted to know about their anesthetic, verified if they understood and asked if they had further questions
PERFORMANCE IMPROVEMENT PLANS
Dr. Cohen is always looking for ways to improve his clinical practice. As a performance improvement tool, he agreed to try out the mnemonic and provide early feedback when evaluating electrophysiology patients. Here were his initial comments:
“The ANESTHETIC mnemonic is an easy-to-use tool. Once the key elements are reinforced, it is easy for the doctor to focus in on the critical elements necessary to achieve better physician-patient communication. If this tool can help my practice, it may be able to help others across all disciplines. I applaud Dr. Giuca for his novel thinking outside of the box, in order to come up with a better ANESTHETIC than those that are used pharmacologically.” ~ Dr. Cohen
CONCLUSION
The need to improve patient communication is well known and discussed in this paper. The ANESTHETIC mnemonic tool attempts to address and overcome the obstacles to teaching and implementing a patient-centered communication strategy. The tool encompasses data from over 40 peer-reviewed journal articles. ANESTHETIC, like any good tool, makes a difficult job easier by accurately consolidating effort. In addition, the teaching strategy that I have devised engages learners. The simulation curriculum allows the students to display the actions and attributes that patients state they are looking for. With the right tools and preparation, patient-centered communication skills can be taught.27,39-41
CLOSING REMARKS BY DR. COHEN
The collaboration between anesthesiologist and electrophysiologist has been solidified at our institution over the past half decade. This partnership has helped with the care of our patients. That being said, there is always room for improvement. The ANESTHETIC tool developed by Dr. Giuca provides a quick and easy method where one may be able to improve the performance of patient-centered communication. Dr. Giuca has described the rationale of such a tool, the way it can be evaluated, and how it can potentially apply to medical students. As a practicing electrophysiologist, I have embraced this tool and am using it in clinical practice.
References
- Fong Ha J, Anat DS, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010 Spring;10(1):38-43.
- Stewart MA. Effective physician-patient relationship and health outcomes: a review. CMAJ. 1995;152(9):1423-33.
- Lipkin M Jr, Quill TE, Napedano RJ. The medical interview: a core curriculum for residencies in internal medicine. Ann Intern Med. 1984;100(2):277-84.
- Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002;287:226-35.
- Fung D, Cohen M. What do outpatients value most in their anesthesia care? Can J Anaesth. 2001;48(1):12-19.
- McKinley R, Middleton JF. What do patients expect from their Doctors? Content analysis of written patient agendas for the consultation. Br J Gen Pract. 1999;49(447):796-800.
- Richards T. Chasms in communication. BMJ. 1990;301(6766):1407-8.
- Makaryus A, Friedman EA. Patients’ understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005;80(8):991-4.
- Olson D, Windish DM. Communication discrepancies between physicians and hospitalized patients. Arch Intern Med. 2010;170(15):1302-7.
- van den Brink-Muinen A, van Dulmen AM, Jung HP, Bensing JM. Do our talks with patients meet their expectations? J Fam Pract. 2007:56(7):559-68.
- Weston WW, Brown JB, Stewart MA. Patient-centered interviewing part I: understanding patients’ experiences. Can Fam Physician. 1989;35:147-51.
- Stewart MA, Brown JB, Weston WW. Patient-Centred Interviewing Part III: Five Provocative Questions. Can Fam Physician. 1989;35:159-61.
- Levenstein JH, Brown JB, Weston WW. The patient-centered clinical method: a model for the doctor-patient interaction in family medicine. In: Stewart M, Roter D, eds. Communicating with Medical Patients. Newbury Park, California: Sage Publications, 1989: 107-20.
- Blanchard CG, Ruckdeschel JC, Fletcher BA, Blanchard EB. The impact of oncologists’ behaviors on patient satisfaction with morning rounds. Cancer. 1986;58(2):387-93.
- MacLeod R. Patients with advanced breast cancer: the nature and disclosure of their concerns [dissertation]. Manchester: University of Manchester, 1991.
- Avis M. Choice cuts: an exploratory study of patients’ views about participation in decision-making in a day surgery unit. Int J Nurs Stud. 1994;31:289-98.
- Middleton JF. Successful consultations: the patients’ agenda. Modern Medicine. 1991; April:183-186.
- Starfield B, Wray C, Hess K, Gross R, Birk PS, D’Lugoff BC. The influences of patient-practitioner agreement on outcome of care. Am J Public Health. 1981;71:127-32.
- Shapiro RS, Simpson DE, Lawrence SL, Talskv AM, Sobocinski KA, Schiedermaver DL. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989;149:2190-6.
- Lev P. Communication with Patients: Improving Satisfaction and Compliance. London: Croom Helm, 1988.
- Little P, Everitt H, Williamson I, et al. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2011;323:908-11.
- Orth JE, Stiles WB, Scherwitz L, Hennritus D, Vallbona C. Patient exposition and provider explanation in routine interviews and hypertensive patients’ blood pressure control. Health Psychol. 1987;6(1):29-42.
- Bass MJ, Buck C, Turner L, Dickie G, Pratt G, Robinson HC. The physician’s actions and the outcome of illness in family practice. J Fam Pract. 1986;23(1):43-7.
- Prideaux D, Alexander H, Bower A, et al. Clinical teaching: maintaining an educational role for doctors in the new health care environment. Med Educ. 2000;34(10):820-6.
- Epstein RM. Assessment in medical education. N Engl J Med. 2007;356(4):387-96.
- Tamblyn RM. Use of standardized patients in the assessment of medical practice. CMAJ. 1998;158:205-7.
- Stillman PL, Swanson DB, Smee S, et al. Assessing clinical skills of residents with standardized patients. Ann Intern Med. 1986;105(5):762-71.
- Simpson M, et al. Doctor-patient communication: the Toronto consensus statement. BMJ. 1991;303(6814):1385-7.
- Smith AF, Shelly MP. Communication skills for anesthesiologists. Can J Anaesth. 1999;46(11):1082-8.
- Peppiatt R. Eliciting patients’ views of the cause of their problem: a practical strategy for GPs. Fam Pract. 1992;9(3):295-8.
- Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;107:692-696.
- Roter DL. Patient participation in patient provider interaction: the effects of patient question-asking on the quality of interaction, satisfaction, and compliance. Health Educ Monogr. 1977;5(4):281-315.
- Bartlett EE, Gravson M, Barker R, Levine DM, Golden A, Libber S. The effects of physician communication skills on patient satisfaction; recall and adherence. J Chronic Dis. 1984;37(9-10):755-64.
- Cole SA. The Medical Interview: The Three Function Approach. St. Louis: Mosby, 1991.
- Greenhow D, Howitt AJ, Kinnersley P. Patient satisfaction with referral to hospital: relationship to expectations, involvement, information-giving in the consultation. Br J Gen Pract. 1998;48(426):911–2.
- Faden RR, Becker C, Lewis C, Freeman J, Faden AI. Disclosure of information to patients in medical care. Med Care. 1981;19(7):718-33.
- DiMatteo MR, DiNicola DD. Achieving Patient Compliance: The Psychology of the Medical Practitioner’s Role. New York: Pergamon Press, 1982.
- Likert R. A Technique for the Measurement of Attitudes. Archives of Psychology. 1932;140:1-55.
- Novack DH, Volk G, Drossman DA, Lipkin M Jr. Medical interviewing and interpersonal skills teaching in US medical schools. Progress, problems, and promise. JAMA. 1993;269(16):2101-2105.
- Maguire P, Fairbairn S, Fletcher C. Consultation skills of young doctors: I—Benefits of feedback training in interviewing as students persist [correction appears in Br Med J (Clin Res Ed). 1986;293:26]. 1986;292(6535):1573-6.
- Maguire P, Roe P, Goldberg D. The value of feedback in teaching interviewing skills to medical students. Psychol Med. 1978;8(4):695-704.

