

Addressing Gender Differences in Cardiovascular Health: Interview with Phyllis E. Greenberger, MSW
 In June 2011, the Society for Women’s Health Research (SWHR) and WomenHeart:The National Coalition for Women with Heart Disease released the 2011 10Q Report: Advancing Women’s Heart Health through Improved Research, Diagnosis and Treatment. In this feature interview, EP Lab Digest speaks with Phyllis E. Greenberger, MSW, President and CEO of the Society for Women’s Health Research, about the top 10 unanswered questions concerning the prevention, diagnosis and treatment of cardiovascular disease (CVD) in women.
In June 2011, the Society for Women’s Health Research (SWHR) and WomenHeart:The National Coalition for Women with Heart Disease released the 2011 10Q Report: Advancing Women’s Heart Health through Improved Research, Diagnosis and Treatment. In this feature interview, EP Lab Digest speaks with Phyllis E. Greenberger, MSW, President and CEO of the Society for Women’s Health Research, about the top 10 unanswered questions concerning the prevention, diagnosis and treatment of cardiovascular disease (CVD) in women.
Tell us about the role of the Society for Women’s Health Research. When and why was it founded?
SWHR was founded in 1990 to focus attention on conditions that disproportionately or exclusively affect women. Before that time, it was becoming obvious to some of our researchers at the NIH that women and minorities were not routinely included in clinical trials. At the time there were very few women included in clinical trials, and there was no attention being paid to women’s health other than reproductive issues. So we went to Congress and asked them to write a letter to the Government Accounting Office (GAO) to investigate the NIH to see whether, in fact, women and minorities were being included in trials, and whether there were line items in the various Institutes such as the National Cancer Institute (NCI) to see if they were looking specifically at female patients. I should note we weren’t referring to diseases such as breast cancer but diseases that can affect both men and women, such as bladder cancer or liver cancer. The Energy & Commerce Committee, then chaired by Rep. Henry Waxman, held a hearing and called all the Institute directors to testify. The Institute directors were told in advance that they would be asked whether their Institute had line item funding to research women’s issues and whether women were included in clinical trials, but not one of them came prepared to answer that. So that was how we got started — you could say it was for us the “shot heard ‘round the world.” After this, there were a number of editorials and articles written on the fact that women were paying half the taxes in this country but the research being performed was mostly on men. So we proposed the question, “If the research is done mostly on men, how do we know it applies to women?” That was one of the first times anyone had brought this up, and it was not met with great enthusiasm from the medical, clinical and research communities. Their general response was, “We’ve always done it this way, and who are they to question it?” It was very controversial and it took some time, and although it’s still not universally accepted, it’s still more accepted than it was at the time.
Describe your collaboration with WomenHeart on this report. How did the report come about?
Actually, I am a founding member of WomenHeart. I used to work with a woman from a PR firm who was interested in getting more attention for sex differences and the inclusion of women in clinical trials. She came to meet with me to see how we could work together, but within a year or so, she had a heart attack. She later told me that she called the American Heart Association to see if they had a support group for women, but they did not — they told her they did not discriminate. At the time, many cardiology associations still believed heart disease was a man’s disease and there was no distinction. So when she got that answer, she came to me and asked if I would work with her to start an organization for women survivors of heart attacks. Of course I said yes, and gave her the bylaws, articles of incorporation, and our funders to help it get off the ground. I’m still on the scientific advisory committee today.
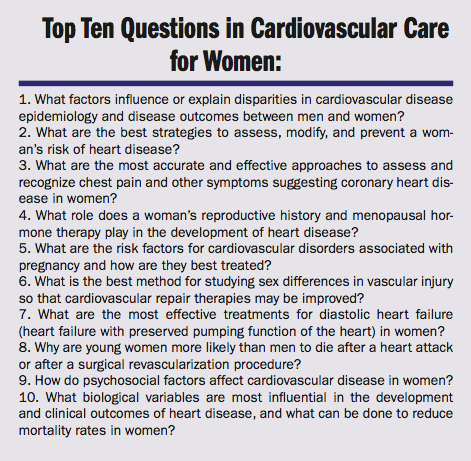
The difference between WomenHeart and SWHR is that WomenHeart is an organization that provides advocacy and education for women with heart disease. SWHR is a research organization; we help fund research and scientists in order to understand sex differences and the implications for prevention, diagnosis, and treatment. In 2006, Nancy Loving, who was the founder of WomenHeart, asked us if we would put together a 10Q Report delineating questions that needed to be answered about women and heart disease. We agreed, and found there were many questions to be raised, so we tried to condense them down to a list of ten. The report was released that year on February 14, Valentine’s Day. However, the report wasn’t widely distributed at the time due to a lack of funding.
WomenHeart now has a different executive director, and a couple of years ago she and I talked about updating the 2006 10Q Report since the first one was done rather quickly. However, this time we wanted to do a more formal investigation as well as a more thorough report. The process took about 2 years, and we had several cardiologists involved.
What are some of the main differences seen between the 2006 and 2011 10Q Reports? What progress in women’s health has been made since 2006?
We included more basic questions in the 2006 report, and some of those original questions were answered. What we realize now is there are even more differences and we need to do even more research. I do think that as a result of the first report, certainly more women are included in clinical trials, which was one of the issues, but we’re still not where we should be.
The 10Q Report notes that only one-third of cardiovascular clinical trials report sex-specific results. How does this negatively impact women’s health in the long-term?
If we don’t have women in all of these trials, then we’re not going to know if differences exist. We’re not saying there are differences in every drug or every diagnostic test, but it’s important to know where there are differences and where there are not. SWHR is having a meeting this September, cosponsored with the Food and Drug Administration, on recruiting more women and minorities in trials. Minorities are equally important as a subgroup in clinical trials. It’s already difficult enough to get people in clinical trials, and it’s that much more difficult to get women in clinical trials because of family priorities such as taking care of children and family, and they need to be approached and spoken to in a different way. We know this from our clinical trials education outreach. There are other issues in terms of recruitment, but the main issue is that there still are not enough women in trials. Even when there are enough women in the trials, very often there is not sex analysis done, so the result doesn’t necessarily show whether there were sex-based differences or not. That’s equally important, of course, and that has been the failure of a lot of clinical trials. Diastolic heart failure apparently affects more women than men, yet the trials at the National Heart, Lung, and Blood Institute (NHLBI) have typically been just men, which begs the question “why?”.
Question #2 in the report addresses the best strategies for assessing a woman’s risk for heart disease. Describe some of the challenges faced in diagnosing and preventing coronary heart disease (CHD) in women.
The first is that there is still a significant segment of the female population that isn’t aware of the fact that heart disease affects them. Also, what we’re seeing and we don’t understand is heart disease in younger women in their 30s and 40s. These patients don’t really believe that they’re having a heart attack — they think it must be something else because they are so young and this shouldn’t be happening to them. I heard a story the other day from a woman who went to the hospital and said, “I think I’m having a heart attack.” The medic said, “you’re too young to have a heart attack,” and this woman said, “No, I’m not, I’ve already had one.” So there’s this lack of understanding that women can get heart attacks and they can get them at any age. There can be different symptoms, of course. Patients tend to think the symptoms will be very dramatic, and that they should be clasping their chest or gasping for breath during a heart attack, but in fact you can have neck, back, or even jaw pain. It’s not always a heart attack, but these are symptoms of a possible heart attack and a lot of people don’t know that. There is also the age-old issue of women taking care of themselves last and denying that they couldn’t be having a heart attack (eg, “I’ll just wait a few minutes and then I’ll be fine”). I think from the women’s point of view, these are some of the issues. From a cardiologist’s or ER doctor’s point of view, there is still, in some cases, a lack of knowledge about symptoms and a tendency to view women’s symptoms as being psychological or as indigestion or stress. We’re still hearing that. Certainly there is a cohort of cardiologists and specialists that are much more aware, but like everything else, it takes time to permeate through the medical and clinical community, so there is still a fair lack of awareness or acceptance.
The points raised in question #5 in the report were especially interesting. Discuss the difficulties health care providers face when cardiovascular disease complicates pregnancy. How does this put women’s health at risk?
We have a network looking into those areas, and new research shows that preeclampsia can possibly portend future heart disease risk. They are also looking at the effect on the fetus, whether it’s male or female, and whether there is an effect there. The whole area of reproduction and association with pregnancy are questions that need to be answered and have been given, only recently, any attention at all. That’s the question but we don’t have the answer.
Why would increased funding in this particular area be beneficial?
On the whole, we have to be able to prevent preeclampsia — it impacts too many women — and our network is actually doing work in this area. They are looking through databases of women who have preeclampsia to see if they have cardiovascular disease. For example, if a woman was more vulnerable to cardiovascular disease because of her pregnancy, then her physician could monitor her, talk to her about it and tell her she has to be aware that if she has certain symptoms, she needs to recognize them or have an electrocardiogram and check it out. It’s really more about education and prevention to understand that there may be issues at this reproductive stage that may increase a woman’s vulnerability later on in life. If it turns out that there is some relation, then that would be the same thing. Women need to understand the symptoms and if they suffer from them, not to ignore them.
Question #9 in the report addresses how psychosocial factors affect women’s health. Tell us more about these psychosocial factors, and why it was important to recognize their significance.
A key element in the 2011 10Q Report focuses on the psychosocial factors of cardiovascular disease. To date, few accounts of medical literature and patient resources have examined the importance of psychosocial issues, particularly in the case of cardiac arrest. Lack of information in this area has unfortunately left both physicians and patients with little guidance. Psychosocial factors, including depression, inadequate social and economic resources, marital stress, etc., are linked to adverse cardiovascular outcomes. Healthcare providers, particularly primary care doctors, need to be cognizant of this and assess a woman’s mental status and psychosocial factors as they relate to cardiovascular disease.
I’ll be interested in learning more about the follow-up and its significance.
We’ll see. Our network is looking at pregnancy issues, and hopefully they’re going to come out with some findings that will be helpful. In terms of the other questions, it really depends on researchers to take any one of these questions seriously and start doing research in this area and with the NHLBI. We know and you know that funding is not good and probably will be cut further, and it will be very difficult for various Institutes to continue to support research in various areas. There needs to be an allocation of the existing funds to reflect the importance and the severity of this issue so that it is not ignored. We realize that there probably is not going to be new money coming in, but a percentage has to be given to those conditions that affect women differently or to make sure that women are in these clinical trials and that we understand the sex differences. I wish I could say that in issuing this report that if I speak to you 3 or 5 years from now, we’re going to have the answers. These answers take a long time and we need funding in order for the researchers to investigate them.
What changes would you like to see made in NIH funding for heart disease and stroke?
I think the allocation of money needs to be different. Again, there will most likely be a cutback. We know that we can’t go to Congress and get more money; I think that would be highly unlikely that that would happen, so we need to be looking at how funding is allocated and make sure that it’s distributed in those areas where it is most needed. I’m not saying that they shouldn’t keep funding men’s research — we want men to live long and be healthy. However, since 50,000 more women a year suffer from cardiovascular disease, I think it’s reasonable that they should get their full share of funding and research.
Tell us about the HEART for Women Act, and why Congress should pass this legislation. Also, what is the WISEWOMAN program?
The WISEWOMAN program requires the Department of Health and Human Services to submit a Congress report on women and heart disease. In addition, we’ve been trying to pass the HEART for Women Act for a number of years but still need a cosponsor. The Heart Disease Education, Analysis, Research, and Treatment for Women Act (HEART Act), S.438, is legislation that seeks to improve the diagnosis, treatment and prevention of heart disease in women by requiring the reporting of sex- and race-based data for new medicines and devices and expanding the Centers for Disease Control and Prevention’s WISEWOMAN screening program for low-income, uninsured women. We’re stalled because we don’t have bipartisan sponsorship. It also requires compliance with the Food and Drug Administration for clinical study safety and effectiveness.
Do you expect to do another 10Q Report update in 5 years?
I think that we’re just going to continue working on this until we see the results of research that really make a difference. When we did the first report, we didn’t know we were going to do the second one, so unless there’s an amazing turnaround, I expect there will still be questions that haven’t been answered as well as other questions that will arise next time. The more research is done, the more questions arise. Nothing is ever definitive with science — there is always a need for more research.
What first steps can health care providers take today to address the recommendations made in the 10Q Report?
I think to some extent, until we have some of these answers, there’s not much they can do. The psychosocial issues can be addressed. Doctors also have to be more attuned to talking to women about the possibility of heart attack. They have to understand and recognize that symptoms are different in men and women. This has to extend to OB/GYNs and primary care doctors as well, because most women are not going to go to a cardiologist unless they’ve already had some heart problems or there are genetic or hereditary factors. In general there needs to be more education in terms of prevention and education, and how women need to be treated differently.
Both men and women have to try to get as much information as they can about conditions so they can ask their doctors the right questions. Patients need to be advocates for themselves, but ultimately the doctor still makes the final decision, and most of us haven’t gone to medical school. The best you can do is to be well educated and pay attention. The 2011 10Q Report is being distributed more widely, and we’re doing our part to get it out to as many physicians and healthcare providers as we can, so hopefully this will have an impact.
For more information, please visit:
www.womenshealthresearch.org
www.womenheart.org

