

An Approach to Transvenous Lead Extraction in Patients With Malfunctioning or Superfluous Leads
Transvenous lead extraction (TLE) is a complex procedure that carries a small but significant risk of life-threatening procedural complications.1 Preprocedural identification of the small group of patients at exceedingly high risk of intraprocedural complications has been challenging. Therefore, decisions related to extraction versus abandonment of noninfected malfunctioning or superfluous leads remain challenging.
In this study, we present 3 patients who underwent TLE for noninfectious indications utilizing an intraprocedural risk stratification approach to guide decision-making regarding lead abandonment versus extraction.
Case Presentations
Case 1:
This patient is a 78-year-old male with a history of aortic valve replacement, atrioventricular (AV) block, and dual-chamber pacemaker implantation 13 years ago, and pacemaker generator replacement 3 years ago. He developed heart failure and moderate cardiomyopathy, likely related to chronic right ventricular (RV) pacing. Additionally, the RV lead pacing threshold had been progressively increasing, causing premature battery depletion. The patient was referred for upgrade to a biventricular pacemaker and RV lead replacement.
Case 2:
This patient is an 81-year-old female with symptomatic sinus node dysfunction requiring dual-chamber pacemaker implantation. After 12 years, she developed severe ischemic cardiomyopathy and underwent upgrade to a biventricular ICD with implantation of new RV and left ventricular (LV) leads, while the old RV pacemaker lead was abandoned. After 5 more years, the ICD RV lead exhibited evidence of lead fracture and the ICD battery became depleted. Complete occlusion of the left subclavian vein was diagnosed on venography. The patient was referred for ICD generator and RV lead replacement.
Case 3:
An 82-year-old female with complete AV block required implantation of a dual-chamber pacemaker. Nine years later, RV lead malfunction was observed and a new RV lead was implanted, while the malfunctioning lead was abandoned. Five years later, the patient developed malfunction of the right atrial (RA) lead, causing loss of sensing and pacemaker syndrome. The patient was referred for lead replacement.
Lead Extraction Technique
In a shared decision-making process, discussions with each patient regarding extraction or abandonment of leads were undertaken to address both the acute risks of TLE and the risks inherent to lead abandonment. Since lead removal was not a must, it was agreed to attempt TLE as long as high-risk techniques (namely, mechanical/laser dissection at the superior vena cava [SVC]-RA junction) could be avoided. Otherwise, the lead(s) would be capped and abandoned.
The TLE procedures were scheduled in the EP laboratory without cardiothoracic surgery backup. All procedures were performed under monitored deep anesthesia with invasive arterial blood pressure monitoring. Tools necessary to stabilize the patient in the setting of severe cardiovascular complications, such as the SVC occlusion balloon and pericardiocentesis, were immediately available. Fluoroscopy was utilized to monitor for intrathoracic bleeding complications, as discussed in a recent report.2
A stepwise approach to lead extraction was systematically employed. Initially, a regular stylet was advanced in the target lead and the active fixation mechanism (when present) was retracted. Simple manual traction was attempted; if this failed, traction was repeated with a locking stylet. If manual traction was unsuccessful, a laser sheath (Philips) was used. Continuous traction on the lead was employed in an effort to use the lead as a ‘rail’ for the laser sheath to dissect over. The laser sheath was advanced over the lead with laser activation at sites of binding adhesions within the subclavian and innominate veins. Upon reaching the SVC, countertraction was applied with the laser sheath while traction was applied to the lead. No laser activation was applied beyond the innominate vein. When the sheath could be advanced over the lead into the RA without laser activation, the extraction procedure was continued, and the laser could be activated beyond that point if needed. If the sheath could not be easily advanced over the lead, the lead was manually retracted while holding the laser sheath in position. If the lead could not be pulled back into the sheath, manual traction was applied to pull the lead-sheath assembly as one unit.
If the lead remained firmly adhered to the SVC, the extraction procedure was halted, and the lead was abandoned. Lead extraction was also abandoned whenever the procedure was perceived by the operator to expose the patient to higher risk based on the intraprocedural assessment and difficulty in extracting. When TLE was not feasible, the lead was capped and abandoned.
Lead Extraction Outcomes
In the first case, the malfunctioning RV lead (active fixation, dwell time 13 years) was extracted using a laser sheath (Figure 1, Video 1). New RV and LV leads were implanted. In the second case, the malfunctioning ICD RV lead (active fixation, dual-coil, dwell time 5 years) was successfully extracted using a laser sheath, which enabled securing venous access for implantation of the new lead. Extraction of the abandoned RV lead (active fixation, dwell time 17 years) was attempted; however, after advancing the laser sheath over the lead within the subclavian and innominate veins, the lead remained tightly bound to the wall of the SVC and could not be freed with manual traction at that point. When laser application at the SVC-RA junction appeared to be necessary for lead removal, extraction efforts were halted and the lead was abandoned. The locking stylet was cut and a protective cap was placed at the proximal end of the lead, which was sutured to the underlying pectoral muscle sheath. In the third case, the malfunctioning RA lead and the abandoned RV lead (both leads were active fixation, 14 years dwell time) were successfully extracted using a laser sheath, and a new RA lead was implanted (Figure 2, Video 2). All patients recovered well without complications and were discharged after a few hours of monitoring.

Video 1
Video 1. Fluoroscopy anteroposterior views of atrial and ventricular pacing leads before (A) and after (B) extraction in Case 1.

Video 2
Video 2. Fluoroscopy anteroposterior views of atrial and ventricular pacing leads before (A) and after (B) extraction in Case 3.
Discussion
Expanding indications for cardiac implantable electronic device (CIED) therapy and improved life expectancy of patients with cardiac disease have led to an exponential increase in the number of devices and leads being implanted. In parallel, the incidence of lead extraction has steadily increased. Today, lead extraction is an integral part of the long-term management of CIED patients.
In patients with CIED-related infections, complete removal of all components of the infected device and leads is necessary to eradicate the source of infection.1 On the other hand, in patients undergoing CIED upgrades or lead revisions, extraction of malfunctioning or superfluous leads is not a must, and decisions related to extraction versus abandonment of leads in these cases remain controversial. While the strategy of lead abandonment obviates TLE procedural risks, it carries short- and long-term risks related to increased risk of venous occlusion in the setting of high lead burden, potential for lead–lead interaction, and the impact of multiple leads crossing the tricuspid valve resulting in valvular regurgitation or functional stenosis. In addition, lead abandonment can preclude magnetic resonance imaging. Importantly, the future risks of potential lead extraction (eg, for CIED-related infections) need to be considered in lead abandonment. The presence of previously abandoned leads has been shown to increase the complexity and risk of the TLE procedure given the increasing lead dwell and lead-tissue adherence.3 Under such circumstances, abandonment might mean that extraction of aged leads is only postponed, while lead removal at an earlier time might pose lower procedural risks.
On the other hand, TLE carries a significant risk of life-threatening complications. SVC laceration and cardiac perforation can lead to rapid hemodynamic collapse and death if detection and treatment are delayed. Therefore, the 2017 HRS expert consensus statement emphasized the importance of immediate availability of safety measures in place, including a cardiothoracic surgical team with access to equipment to perform emergent thoracotomy.1 Nonetheless, it is important to note that, using contemporary extraction tools and techniques, TLE can be performed safely in the vast majority of patients, and the risk of intraprocedural complications requiring immediate surgical intervention is small (<1%). However, identifying the small group of patients at exceedingly high risk for whom the immediate availability of a surgical team is necessary remains challenging. While various approaches to risk stratification have been proposed, correlation with safety has been lacking, and none of the risk stratification models have been validated to prospectively guide procedural planning.
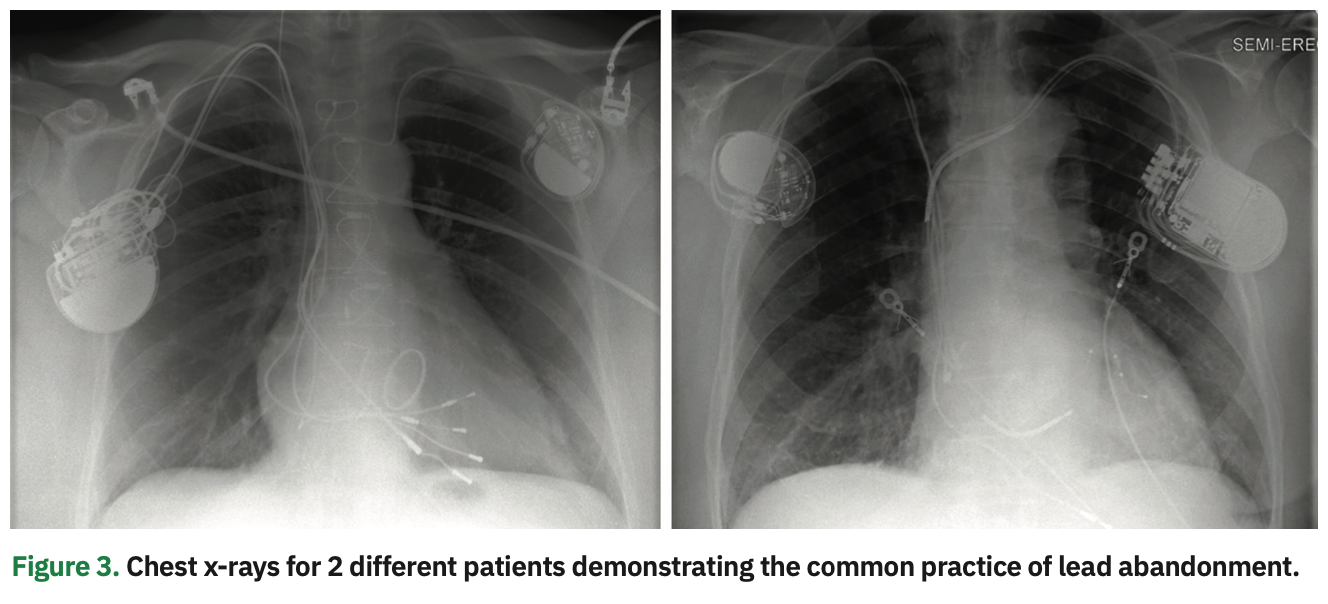
As a consequence, TLE procedures have been considered a category of high-risk interventions, mandating the immediate availability of a multidisciplinary team including a cardiothoracic surgeon, cardiac anesthesiologist, perfusionist, and nursing personnel. This has resulted in increased procedural cost, inefficiency, and resource utilization that are not be feasible at many institutions. The increased procedure complexity has significantly curtailed incorporation of TLE programs beyond a relatively limited number of experienced lead management centers, and hence, there is a limited proliferation of TLE skills among EP trainees. Furthermore, access to care has been hindered for many patients who would benefit from lead extraction for noninfectious indications. Not infrequently, these patients are managed by leaving the nonfunctional leads and adding new leads on the same or contralateral side with no attempt at removing the lead that otherwise could be removed with very minimal added risk. In fact, it is estimated that almost 1 in every 4 patients requiring extraction for CIED infection had a previously abandoned lead in place, a manifestation of the common practice of lead abandonment (Figure 3).3
At our institution, we utilize a unique approach to lead management in patients with noninfectious indications of lead extraction. In this patient population, lead extraction is preferred to abandonment, as long as the procedure can be performed safely without exposing the patient to an unacceptably high risk. Since preprocedural risk stratification schemes are often of limited value in guiding decision making, we judge procedural risk only after an initial attempt at TLE is undertaken. When extracting the lead proves difficult or requires the use of high-risk techniques (such as laser application and mechanical dissection at the SVC-RA junction), lead abandonment is preferred. A recent study found that a large proportion of leads could be successfully and safely extracted without such high-risk techniques.4 This approach can potentially help guide resource utilization and optimize the balance between efficacy, safety, and efficiency in lead extraction practice, and facilitate the development of TLE programs at more institutions. This can also help disseminate TLE skills, enable more electrophysiologists to perform at least “low-risk” TLE procedures, and expand lead management options to a larger proportion of patients.
It is important to note that our approach to TLE carries several limitations. First, it can potentially expose the patient to a repeat extraction procedure; nevertheless, it then would offer the patient the advantage of making a more informed decision regarding the realistic procedural risk. Second, when a lead is abandoned after a failed extraction attempt, the locking stylet is cut and left inside the lead, which can pose challenges to extraction of the lead in the future. However, in our experience, using lead extenders and the femoral approach to TLE can overcome such challenges.
Conclusion
Vascular laceration and cardiac perforation are the most serious complications of TLE, and frequently require emergent surgical intervention. Identifying the small group of patients at exceedingly high risk of procedural complications remains challenging and reliable preprocedural indicators of risk are lacking. On the other hand, treating TLE candidates as a homogenous high-risk group entails denying many patients an attempt at TLE or mandating the recruiting of vast resources for a procedure that can be performed successfully using safe techniques in the majority of patients. Our approach prefers lead extraction over lead abandonment whenever the extraction procedure can be performed safely without exposing the patient to an unacceptably high risk. Such an approach can potentially simplify adoption of TLE at a larger number of programs, rendering TLE procedures more efficient and less resource-intensive, and expanding lead management options to a larger proportion of patients.
Disclosures: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr. Issa has no conflicts of interest to report regarding the content herein.
Connect with Dr. Issa on Twitter at: @ZiadIssaMD
Test your knowledge: Bonus quiz on this topic available here!
References
1. Kusumoto FM, Schoenfeld MH, Wilkoff BL, et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 2017;14(12):e503-e551. doi: 10.1016/j.hrthm.2017.09.001
2. Issa ZF, Issa TZ. Utility of fluoroscopy alone for monitoring of intrathoracic bleeding complications during transvenous lead extraction. J Cardiovasc Electrophysiol. 2021;32(6):1724-1732. doi: 10.1111/jce.14995
3. Hussein AA, Tarakji KG, Martin DO, et al. Cardiac implantable electronic device infections: added complexity and suboptimal outcomes with previously abandoned leads. JACC Clin Electrophysiol. 2016;3(1):1-9. doi: 10.1016/j.jacep.2016.06.009
4. Issa ZF. Transvenous lead extraction in 1000 patients guided by intraprocedural risk stratification without surgical backup. Heart Rhythm. 2021;18(8):1272-1278. doi: 10.1016/j.hrthm.2021.03.031

