


The Cardiovascular Shift to the Outpatient Setting
Is your organization prepared for the shift of cardiovascular procedures to the ambulatory surgical center (ASC)? If you have not had these discussions, developing a strategic plan will be crucial, as the shift has already begun.
In 2018, it was estimated that 10% of all cardiovascular (CV) procedures were performed in the ASC.1 A current market analysis estimates a greater than 30% increase in CV volume by the mid-2020s, and some estimates are even higher with the introduction of the additional approved procedure codes. Navigating the clinical, financial, and operational considerations requires detailed knowledge of Medicare’s covered procedures, patient selection criteria, and common barriers to implementation. Corazon, Inc., works diligently to stay on the leading edge of Medicare updates and other important factors influencing the shift in settings of care, and we believe it is imperative that hospitals be prepared for what is to come.
Cardiovascular Covered Procedures
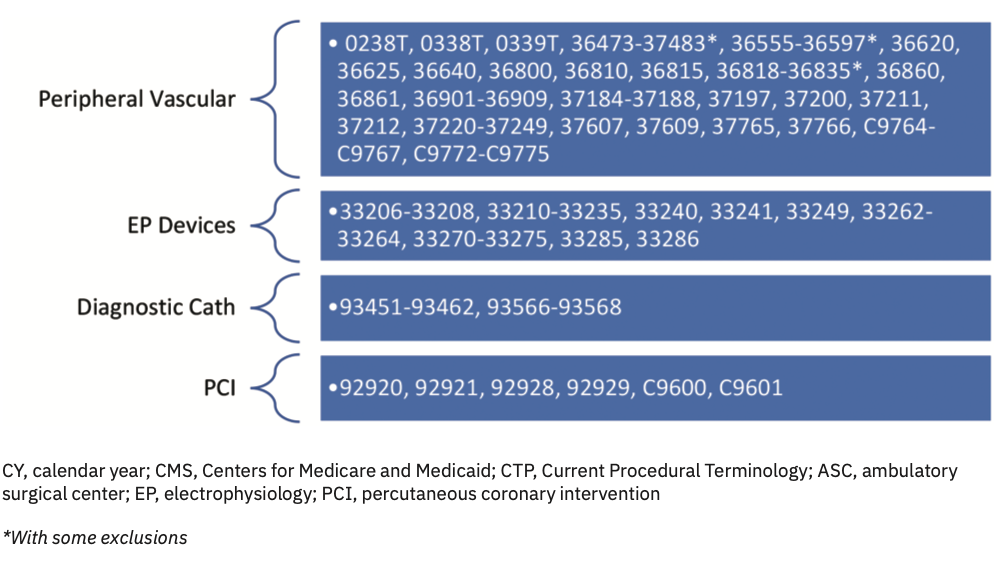
The ability to perform surgical, diagnostic, and interventional procedures in the ASC is due largely to the significant advances and current innovations in technique, devices, and pharmacology, coupled with a high rate of positive outcomes and a minimal amount of major complications.2 Over the last 10 years, the Center for Medicare & Medicaid Services (CMS) has gradually recognized these clinical advances by adding cardiovascular procedures to the covered procedure list (CPL), beginning with peripheral vascular procedures. It has only been in the last 5-7 years, however, that CMS has permitted and reimbursed for device implants, diagnostic cardiac catheterizations, and low-risk percutaneous coronary intervention (PCI) in the ASC setting (see Figure 1 for a list of CMS-approved CV procedures by CPT code in an ASC).
Patient Selection
Appropriate patient selection is vital for an ASC. Patient selection can have an impact on patient safety, efficiency, and ASC reportable events. Determining suitability depends on a variety of factors, such as a patient’s medical history or the anticipated type of anesthesia. Other considerations include the type of ambulatory setting (i.e., freestanding ASC, hospital-based outpatient department, office-based lab) and social factors, such as the availability of a responsible person to care for the patient at home.
Ultimately, the decision to furnish services in the ASC setting should be based on the physician’s clinical assessment of the patient’s risk factors. In the final rule, CMS acknowledges the importance of making PCI payable in the ASC setting, stating that “a majority of Medicare beneficiaries may not be suitable candidates to receive these procedures in an ASC setting due to factors such as age and comorbidities.”3 In a 2014 consensus statement, reiterated again in 2020, the American College of Cardiology, American Heart Association, and the Society for Cardiovascular Angiography and Interventions (SCAI) provided guidance for excluding patients and cardiac lesions that were inappropriate for a setting without cardiac surgery backup.4,5 In addition, the ASC will likely have further exclusions such as high body mass index, history of malignant hyperthermia, difficult intubation, etc. Regardless of the site of service, the expectation is that the patient will receive the same standard quality of care.
Common Barriers to Implementation
Cardiovascular care is very complex. Utilizing a multidisciplinary team to formulate a strategic plan for the merging of cardiovascular services to the ambulatory surgery arena will be imperative to anticipating and overcoming inevitable challenges. Having a proactive approach will help ensure that the organization is prepared for success.
Regulatory and accreditation requirements for ASCs can be quite complex. Offering cardiovascular services in an ASC is state-specific and state regulations will supersede national CMS approval. Some states require a Certificate of Need, while others are regulated by the state department of health. Third-party specialty-specific (i.e., cath lab) accreditation is required in some states and not in others. In addition, some states will require a detailed application to add a new service line. Although Medicare has approved these procedures to be performed in an ASC, Corazon recommends reviewing state regulations to ensure these CV procedures are allowable. For example, roughly 40% of states currently allow PCI procedures to be performed in an ASC.
Equipment and space requirements can be quite extensive. Capital equipment requirements and supplies can cost upwards of $1 million. Plus, facility costs for the square footage required for the necessary fixed equipment in the procedural room and an adjacent control room can be as much as two normal size operating rooms. While it is an additional revenue stream, cardiovascular care is not inexpensive. Some may even argue that the low number of patients that meet such rigorous criteria will not justify such an expense. To assess if shifting CV procedures to an ASC is financially feasible, Corazon recommends a thorough market analysis to determine volume potential, and a financial business plan to determine investment costs and return. As a rule of thumb, an ASC will need to perform at least 800 cases to make a solid business case to invest in a cath lab.
Staffing requirements for a cardiac team in the ASC can be challenging. Despite the attractive schedules typically offered in an ASC (e.g., no nights, no weekends, no call), salary rates tend to be lower, which only adds to the difficulty in recruiting experienced personnel. The success of the program requires qualified and experienced cardiology-trained nurses along with dedicated radiologic and/or cardiac technologists. In Corazon’s experience, the typical staffing in an ASC cath lab is one registered nurse and one technologist. The dedicated cardiac staffing model often differs from the traditional staffing culture in an ASC, where the clinical staff can be assigned to any surgical procedures. ASCs performing PCI must also align with qualified physicians. Although credentialing decisions are site-specific, SCAI strongly recommends interventional fellowship training, board certification, and a minimum annual volume of at least 50 PCI procedures per operator.4,5
Conclusion
There is no denying the existing limitations involved in shifting cardiovascular procedures to the ASC setting. However, there are many important stakeholders that are incentivized by making such a shift happen. First, patients are attracted by the ease of access, affordability, and timely and efficient process of ASC care. Subsequentially, increased patient satisfaction is to be expected. Second, physicians are afforded greater control over their practice through the ease of scheduling, greater staff expertise, and improved efficiency and productivity found in an ASC setting. And third, payors are demanding high-quality, low-cost services, which ASCs are known to provide. Once these cardiovascular procedures move to the ASC, it is unlikely that these procedures will move back. How will your hospital be part of the change?
 To learn more, visit www.corazoninc.com or call (412) 364-8200. To reach the authors, email Kristin Truesdell at ktruesdell@corazoninc.com and Lori Griffith at lgriffith@corazoninc.com
To learn more, visit www.corazoninc.com or call (412) 364-8200. To reach the authors, email Kristin Truesdell at ktruesdell@corazoninc.com and Lori Griffith at lgriffith@corazoninc.com
References
1. van Biesen T, Johnson T. Ambulatory surgery center growth accelerates: is Medtech ready? Bain and Company: Brief. September 23, 2019. Accessed February 11, 2022. Available online at https://www.bain.com/insights/ambulatory-surgery-center-growth-accelerates-is-medtech-ready/
2. Masoudi FA, Ponirakis A, de Lemos JA, et al. Trends in U.S. cardiovascular care: 2016 report from 4 ACC National Cardiovascular Data Registries. J Am Coll Cardiol. 2017; 69(11): 1427-1450.
3. Centers for Medicare & Medicaid Services. Medicare program: changes to hospital outpatient prospective payment and ambulatory surgical center payment systems and quality reporting programs; revisions of organ procurement organizations conditions of coverage; prior authorization process and requirements for certain covered outpatient department services; potential changes to the laboratory date of service policy; changes to grandfathered children’s hospitals-within-hospitals; notice of closure of two teaching hospitals and opportunity to apply for available slots. Federal Register. November 12, 2019. Accessed February 11, 2022. Available online at https://www.federalregister.gov/documents/2019/11/12/2019-24138/medicare-program-changes-to-hospital-outpatient-prospective-payment-and-ambulatory-surgical-center
4. Dehmer GJ, Blankenship JC, Cilingiroglu M, et al. SCAI/ACC/AHA Expert Consensus Document: 2014 update on percutaneous coronary intervention without on-site surgical backup. J Am Coll Cardiol. 2014 Jun 17; 63(23): 2624-2641. doi: 10.1016/j.jacc.2014.03.002. Epub 2014 Mar 17. Erratum in: J Am Coll Cardiol. 2014 Jul 22; 64(3): 335.
5. Box LC, Blankenship JC, Henry TD, et al. SCAI position statement on the performance of percutaneous coronary intervention in ambulatory surgical centers. Catheter Cardiovasc Interv. 2020 Oct 1; 96(4): 862-870. doi: 10.1002/ccd.289915
