


Why Is My Lab’s PCI Volume Decreasing?
 In this “Conversation in Cardiology,” Dr. Carl Tommaso asks, “Since 2006, the number of percutaneous coronary interventions in the United States is down 39% (963,000 procedures in 2006, 589,000 in 2010), with an estimated 10-15% decrease in each of 2011 and 2012.”
In this “Conversation in Cardiology,” Dr. Carl Tommaso asks, “Since 2006, the number of percutaneous coronary interventions in the United States is down 39% (963,000 procedures in 2006, 589,000 in 2010), with an estimated 10-15% decrease in each of 2011 and 2012.”
What do you feel are the reason(s) for this?
- Bad publicity given to interventional cardiology, because of suspected cases of fraud and abuse.
- Cardiologists focusing on structural heart disease rather than coronary disease.
- COURAGE trial results: increased use of medical therapy.
- Decreased reimbursement.
- Fear of RAC audits.
- Implementation of Appropriate Use Criteria.
- Increased affiliation of cardiologists with hospitals, reducing fee-for-service incentive.
- Patient wariness about undergoing invasive procedures.
- Reduction in the incidence of coronary disease.
- Referring physicians (internists and non-invasive cardiologists) less likely to refer for cath and intervention.
- Other.
I circulated this question to my list of cath lab experts and provide their answers for you here. As with all our conversations, these are the opinions of the authors and published with their permission. At the end of the discussion, there is synopsis and review by Dr. Tommaso, who posed the problem to us.
Mort Kern from Long Beach, California:
My view is that the reduction is of course multi-factorial, but weighted to the following: 1) Appropriateness and fear of consequences; 2) COURAGE trial erroneous conclusions; 3) Purchase of medical groups and reduction of fee-for-service incentivization; 4) Success at coronary artery disease control and reduction through societal behavior and medical treatment.
Peter Ver Lee from Maine:
Our own volume has decreased by 17% over this time. We have a stable, captive population. Because of our geography, very few patients in our service area go to heart centers with PCI capability elsewhere in Maine and fewer go to Canada. The number of interventional doctors and cath labs has not changed. We have always practiced according to what I would call a traditional, conservative, New England style.
I think the main reason for the decline in volume is the wider penetration of statin use, better risk factor control and the emergence of drug-eluting stents. Our conservative style is perhaps the explanation for the lower fall in volume as a percentage. We started out at a lower point and had a shorter distance to fall. In the last few years, however, the volume has been much flatter, only 2-3% decrease annually.
Greg Dehmer from Temple, Texas:
In some respects, the decrease is an example of “Little’s disease”: a little bit of this and a little bit of that or, in other words, it is related to many of the 10 factors listed. I do think Mort’s top 4 are the largest factors.
If you start in 2006, we also need to consider the effect of drug-eluting stents reducing the occurrence of restenosis, despite the chaos of late 2006 and the hype over stent thrombosis. We are now down to single-digit rates of restenosis.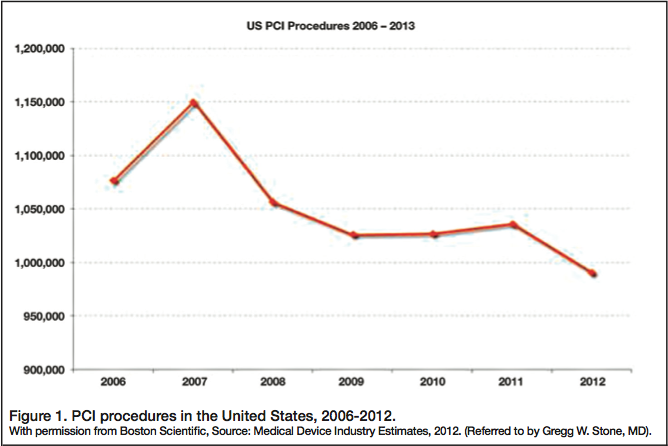 Gregg W. Stone from New York City:
Gregg W. Stone from New York City:
The decrease is not that bad, but still concerning (and misguided) (see Figure 1).
Mladen I. Vidovich from Chicago, Illinois:
Clearly, we have a demographic transition with increase in the older population (Figure 2) and a concurrent epidemiological transition of declining prevalence of CAD (Figure 3). In 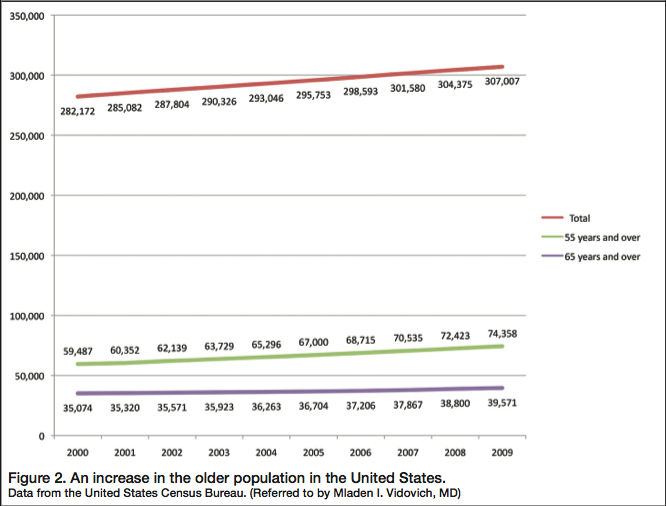 a ballpark unadjusted look, it appears that there are other factors in play beyond just simple secular trends. Perhaps the cumulative number of diagnostic cath/PCI over time impacts its future use/penetration, but we need a good statistician/epidemiologist to confirm that.
a ballpark unadjusted look, it appears that there are other factors in play beyond just simple secular trends. Perhaps the cumulative number of diagnostic cath/PCI over time impacts its future use/penetration, but we need a good statistician/epidemiologist to confirm that.
Lloyd W. Klein from Chicago, Illinois:
I also agree that access to care is probably the number-one factor. Note that Gregg’s graphic takes 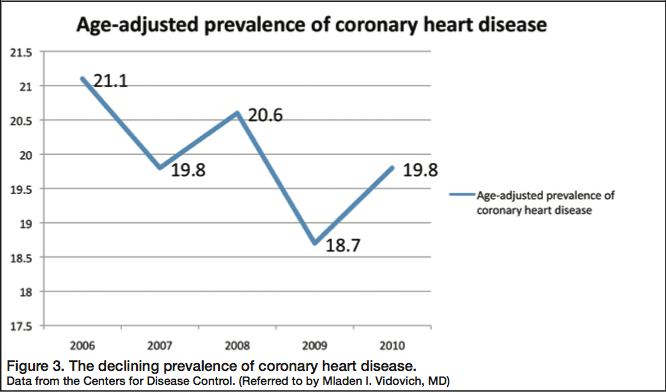 a dip just when the economy did, in 2008. People lost their jobs, and with that loss, insurance.
a dip just when the economy did, in 2008. People lost their jobs, and with that loss, insurance.
Another factor is the aging of our population and a shift to federal government-paid insurance. I do not think that many of the laudable reasons why the PCI volume maybe ought to have decreased is the reason why it did. Once the patient gets into the system, there are good reasons and bad ones why it is tough to keep them out of the lab and a stent from being deployed, but I believe the bad ones typically win out in usual practice. Sorry, I am a cynic.
 Although some primary doctors see themselves as the patient’s protector, and keeping them away from us is their primary goal, I do not think this works so often as to explain Gregg’s graphic (Figure 1). My guess is that repeat procedures over this time frame are decreasing. What used to be an “annuity” is now quite uncommon.
Although some primary doctors see themselves as the patient’s protector, and keeping them away from us is their primary goal, I do not think this works so often as to explain Gregg’s graphic (Figure 1). My guess is that repeat procedures over this time frame are decreasing. What used to be an “annuity” is now quite uncommon.
Bonnie Weiner from Worchester, Massachusetts:
In the current economy, there is a general sense, now apparently corroborated, that patients are not accessing the health care system as much. Probably due to multiple factors, but including concern over taking time off, even if they have health insurance, not having insurance, or not having jobs where dollars are prioritized elsewhere. One would think that ultimately that would result in an increase in acute procedures. There may be significant geographic variation in this and warrants further inspection.
Ted Bass from Jacksonville, Florida: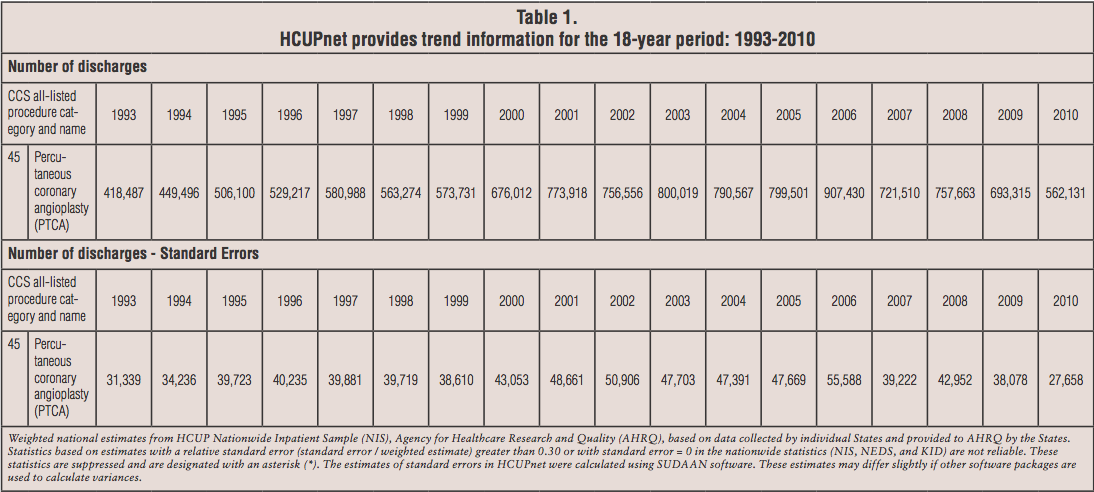 I have attached the AHRQ data (see Table 1). There has been some question that the counting methodology has changed since the peak years in the mid-2006 era, eliminating some “double dipping” on single cases. There are Centers for Disease Control data out there suggesting a less robust, but still significant, decline in procedure volume. I have also attached CMS data and an interesting paper involving many of the issues you bring up. It is hard to get one’s hands around the actual number, but appropriateness analysis seem to imply that currently well >70% of PCI are in the non-elective (ACS) setting and the decrease in numbers probably related to a falloff in the elective cases, suggesting many of the reasons you list might be on target.
I have attached the AHRQ data (see Table 1). There has been some question that the counting methodology has changed since the peak years in the mid-2006 era, eliminating some “double dipping” on single cases. There are Centers for Disease Control data out there suggesting a less robust, but still significant, decline in procedure volume. I have also attached CMS data and an interesting paper involving many of the issues you bring up. It is hard to get one’s hands around the actual number, but appropriateness analysis seem to imply that currently well >70% of PCI are in the non-elective (ACS) setting and the decrease in numbers probably related to a falloff in the elective cases, suggesting many of the reasons you list might be on target.
Riley et al1 confirms recent speculation that PCI volume has begun to decrease. Although rates of CABG have waned for several decades, all forms of coronary revascularization have been declining since 2004. This all has very interesting implications on training volume numbers, competency and certification volume requirements, and manpower distribution, as well as patient access to primary PCI, etc.
Carl Tommaso from Chicago, Illinois:
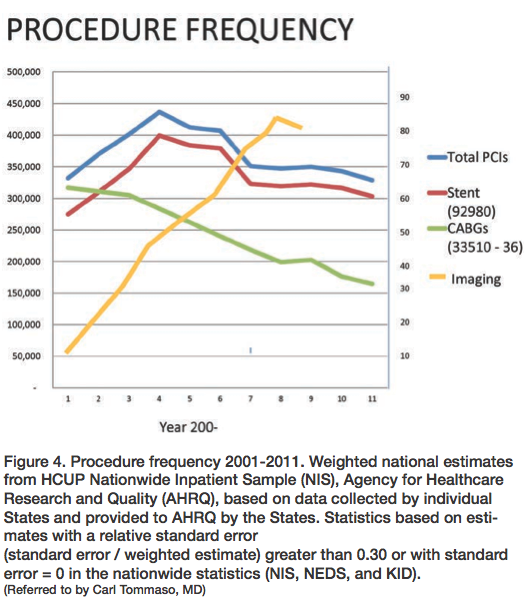
Figure 4 (source: Wayne Powell, SCAI) shows procedural frequency of the last few years. This data eliminates the double counting that plagued the earlier numbers.
Gregg W. Stone from New York City:
This “double-counting issue” has never been completely explained, or at least it doesn’t seem to have made an impact on other data sources. As you can see, industry sources and hospital marketing data keep coming up with much higher numbers.
Jimmy Tcheng from Raleigh, North Carolina:
I would add cigarette taxes, and the resulting drop in tobacco consumption, to the list of contributors to the reduction. Better medications, advancing technologies (DES), greater compliance, improved imaging, clinical trials science, AUC / Hawthorne effect, and administrative (counting) issues round out my list.
Kirk N. Garratt from New York City:
It seems the decline has been most pronounced in elective patients, but I sense the rate of ACS PCI is down some, too. Ted, you hit an important item: maintaining competency is harder than ever if it’s just a numbers game. At my place, the shoe pinches most around emergency cases. State regulations say you need 75 cases, of which 11 are emergencies, to maintain competency. In a hospital with a dozen interventionalists and corralled by PCI-capable places, it’s tough to come up with enough acute patients.
Aaron Kaplan from Lebanon, New Hampshire:
I would add dual antiplatelet therapy (DAPT) confusion. This is defined as confusion/concern on the part of patients and their primary physicians over DAPT management. As a group, I do not believe the interventional community is doing a good job supporting our primary care/referring physicians (PCP) regarding DAPT. As a result there are many patients on indefinite DAPT. Without our clear guidance, the PCP is in a real bind and frets when confronted with a situation that may require discontinuation. This adds complexity and anxiety on the part of the PCP, driving a more conservative approach when managing these patients.
Samuel M. Butman from Arizona:
My thoughts (as I am a bought physician working for a hospital) are that the decrease in volume is due to: 1) Cardiologists focusing on other things rather than coronary disease, more cardiologists (not pointing at you or me directly) sitting at their desks doing computer EMR, CPOE entry instead of getting radiated; 2) Decreased reimbursement; 3) Increased affiliation of cardiologists with hospitals, reducing fee-for-service incentive; 4) Reduction in the incidence of coronary disease.
Coronary heart disease is on the decline and that may be countering the groundswell of excitement about the expected growing baby boomers, i.e. you and I, yet again. In addition, I think docs are retiring earlier and more are looking at other business platforms, be it in medicine or outside (property, spouse working, less divorce activity so less need to make more money than is reasonable (yes, I made up the last one).
John Bittl from Ocala, Florida:
For a look at larger trends in medicine, please see the article entitled, “Doctor Visits Dropping, New Census Figures Show.” This was written by Sabrinia Tavernise and published in The New York Times on October 1, 2012. It states, “Americans of working age are going to the doctor less frequently than they were 10 years ago, according to a new report by the Census Bureau. In 2010, people age 18 to 64 made an average of 3.9 visits to doctors, nurses and other medical professionals, down from 4.8 visits in 2001, said the report, which was released on Monday. The precise reasons for the decline were unclear...”
John W. Hirshfeld, Jr from Philadelphia, Pennsylvania:
This has been a valuable discussion. I would add a couple of additional thoughts. Enlightened case selection is increasingly informed by many excellent clinical trials. With respect to stable patients (patients with acute coronary syndromes are a different group), these trials have told us a number of things that we did not know in 2006. These include:
- Not all stenoses need to be “fixed.”
- “Fixing” hemodynamically insignificant stenoses is commonly detrimental.
- “Fixing” asymptomatic stenoses preemptively in patients planned to undergo non-cardiac surgery is rarely beneficial.
- Stenoses that are highly technically challenging and associated with substantial risk (high SYNTAX score) should have treatment selection based on the balance of the risk-benefit relationships of all potential treatment modalities [both revascularization (EUROScore) and non-revascularization strategies].
The aggregate effect of these emerging concepts has led rational operators to realize that some patients who, in earlier times, would have been considered appropriate for interventional treatment are actually unlikely to be benefited and may be harmed. This has taken these patients out of the “interventional pool” and is likely, along with other factors mentioned by others, a contributor to the overall decline. Finally, I hope that our profession is sufficiently honorable that declining reimbursement is not affecting our case selection.
Mike Lim from St. Louis, Missouri:
I think it would be worthwhile to parallel the decrease in PCI with the decrease in CABG that likely is attributed to risk factor treatment and significantly low restenosis rates. I have thought for quite some time that smoking and restenosis are definitely “good for business”! I am not sure that there is a measurable change from appropriateness criteria or “over-stenting” scrutiny. COURAGE definitely has led non-interventionalists and PCPs to believe that sending patients to cath with symptoms and/or an abnormal stress test is no longer a given. There has been much debate and strong suggestions that sending patients to cath just leads to them “getting a stent” and they feel that this doesn’t help!
Final remarks from Dr. Tommaso:
I would like to thank everyone for contributing their responses to the question concerning the reasons for the decline in the number of PCIs over the last several years. Figure 4 demonstrates the answer to Mike Lim’s question (numbers are different because this is Medicare-only numbers).
The reason I posed this question is that I recently chaired the AMA-PCPI/Joint Commission Symposium on Overuse of PCI. The numbers concerning the decline in PCI were important, but the issue obviously was why the decline occurred. Was it contributed to by a decrease in “overuse”? [A podcast can be found at: National Summit on Overuse Podcasts: Heart vessel stents (percutaneous coronary intervention or PCI): Carl L. Tommaso, MD, North Shore University Health System, https://tinyurl.com/TommasoPodcast].
To make things more controversial, I would like to respond to some of the suggestions of the causes of the decline of PCI.
As to the suggestion that the decline in smoking and use of statins has contributed to the decline in coronary disease, undoubtedly it is true; however, the decline in smoking extends for the last 20 years and statins have been around greater than 25 years, so their impact on the decline in frequency of PCIs should have been more gradual and not as abrupt over the last three or four years. In addition, these factors may be counterbalanced by the aging of the population, the increase of diabetes, and the increase in obesity.
Similarly, to suggest that drug-eluting stents were the cause of the decline of PCIs means this would have happened sooner after their introduction. It was also felt that the use of drug-eluting stents has increased the frequency of PCIs, because of increased indications for the procedures and tackling more complex disease, which was the case right after their introduction.
As far as insurance issues and the decline in the economy as reasons for the decline in PCI, the decrease of PCI in Medicare beneficiaries declined at a similar rate, suggesting that being covered by medical insurance may not have been a major issue. Although the decline in the economy affected the whole of the population, the Medicare age population was probably less affected. The same factors that affect the working population may not affect the retired population in terms of taking time off from work, etc. The fact that people are seeing their physicians less is an interesting cofactor, and no reasons are given. Perhaps this is partly due to the skepticism the public has developed around medicine, and/or the prevalence of alternate care.
So, as Greg Dehmer said, this is probably the “Little Phenomenon,” a little bit of us doing the right thing and adhering to guidelines and AUC, de-incentivization due to hospital employment, improved methods of non-invasive treatment, and decline in the prevalence of CAD.
Editor’s final comment
I think this conversation helps us understand the perceptions of interventionalists on how the change in our practice regarding PCI is occurring and what we might expect in the future. Regardless of these opinions and facts, we should be doing the best job we can in the best way we can for the best reasons known.
--Mort Kern
Reference
1. Riley RF, Don CW, Powell W, Maynard C, Dean LS.Trends in coronary revascularization in the United States from 2001 to 2009. Recent declines in percutaneous coronary intervention volumes. Circ Cardiovasc Qual Outcomes 2011; 4: 193-197.
The Mumford Files
by Phillip Mumford, RCIS
Starting an Interventional Program
Director Cath Lab
Palestine Regional Medical Center
Palestine, Texas
For most people working in interventional labs, not having an interventional program is hard to imagine. Believe it or not, there are still many labs out there only doing diagnostic procedures, and many of them are considering how to add interventional procedures to their lab. Starting an interventional program isn’t an easy task, but with a staff that is willing to learn, it can be done effectively. My own experience has shown that a diagnostic cath lab can begin to do interventional procedures successfully after as little as three months of serious training and work. This kind of transition involves a great deal of learning on the part of the staff, with a lot of preparation on the administrative side as well.
One of the first things to accomplish is finding a cardiologist willing to help start an interventional program. It takes great deal of patience from the cardiologist, a trait that might be overlooked as the facility moves to hire. Starting the training process for the staff needs to take place quickly. Not only does the staff need to learn the process of doing interventions, but they also need to learn to effectively operate new equipment (intravascular ultrasound, the AngioJet, Impella, etc.) that is needed to accomplish successful outcomes. Remember, utilizing company representatives can be a great tool.
Once you have an experienced trainer giving staff the needed education, the facility can start with the administrative aspect. If you do not have open-heart surgery at your facility, I recommend making an agreement with the closest facility that offers it. The initiating facility should take their management staff, as well as the cardiologists, to the receiving facility in order to set up a program that benefits patients with a safe and speedy transfer. Remember not to leave out the transferring service. You will also need to set up an agreement with an ambulance service, EMS, etc., as well. The service transferring the patients will also need some training to make sure their staff knows how to effectively take care of any equipment used to transfer patients (Impella, intra-aortic balloon pump, sheaths, etc.) Some areas may require a staff member from the transferring cath lab to transfer with patient.
Facilities often forget that the new interventional program will also need to have its policy and procedures added to the hospital’s current ones, which is why I recommend that the facility use an experienced person to manage the program development. In addition to policy and procedures, the cath lab will also need to put together competencies for the new procedures as well. The entire staff should be well trained and given every opportunity to discuss the training program with the trainers. New medications will be used as well, which should be discussed with your cardiologists and medical director. In addition to the pharmacy, ask the representatives to come in and train staff, and stock for usage.
As I noted, asking representatives to provide education for their product can be a good resource. Most of the supply companies have their own onsite training for many different aspects of interventional procedures and this should be taken advantage of.
I have presented a brief explanation of what is involved when starting an interventional program. Of course, there is more that has to be accomplished, but starting with these few items will get your program off the ground. Just remember that your staff needs to be fully trained in every aspect of interventions, in addition to getting all of your administrative paperwork in order.
If you have any questions or concerns, please don’t hesitate to contact me. I would be happy to share some additional ideas about starting an interventional program.
If you have a subject you would like covered or an area of interest, please contact Phillip Mumford, RCIS, at p_mumford@aol.com.
Follow Phillip on Twitter.com
@phillip_mumford
