


ADVERTISEMENT
VEITHSymposium: Atherectomy for Lower Extremity Occlusive Disease: What to Use and When
There is an increasing comfort level with stenting in the lower extremities. Does atherectomy completely negate the need for a stent?
Yes. Atherectomy allows the operator to achieve stentlike results without having to leave a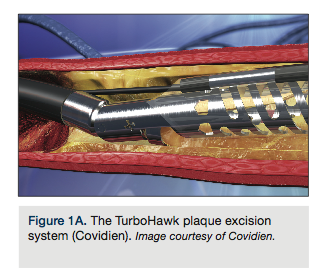 foreign body behind. We are finally getting reasonable data demonstrating its efficacy. Today, there is a much greater interest in atherectomy as a primary therapy and not just as some isolated, niche intervention. At the VEITHSymposium, a casual audience vote had an equal number of people voting for atherectomy and stenting, which is quite different than what we have seen in the past. Many people did not believe that atherectomy had a distinct role. Now, good, core lab-adjudicated, controlled, one-year data, showing there is a distinct advantage for the atherectomy device, were presented during the late-breaking trials at VIVA 2012.1 Our single-center prospective data extending out to 3 years with primary atherectomy
foreign body behind. We are finally getting reasonable data demonstrating its efficacy. Today, there is a much greater interest in atherectomy as a primary therapy and not just as some isolated, niche intervention. At the VEITHSymposium, a casual audience vote had an equal number of people voting for atherectomy and stenting, which is quite different than what we have seen in the past. Many people did not believe that atherectomy had a distinct role. Now, good, core lab-adjudicated, controlled, one-year data, showing there is a distinct advantage for the atherectomy device, were presented during the late-breaking trials at VIVA 2012.1 Our single-center prospective data extending out to 3 years with primary atherectomy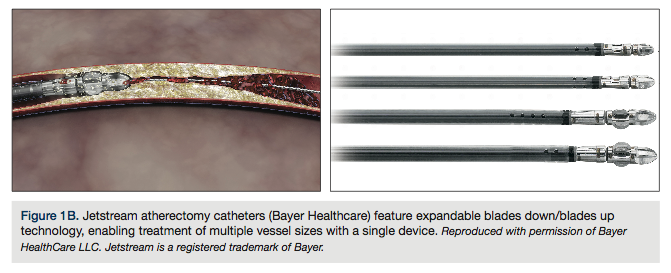 therapy reinforce this advantage.2 Its use comes without the disadvantage of having to leave a stent behind.
therapy reinforce this advantage.2 Its use comes without the disadvantage of having to leave a stent behind.
Aside from any lack of data, why was atherectomy previously viewed with such hesitation?
I think some of the early trials with atherectomy were very flawed, associated with physician bias and conflict of interest. Also, quite candidly, there is an expense to the use of these devices. It costs more to do atherectomy than to put in a balloon and 1-2 stents, and it takes more time.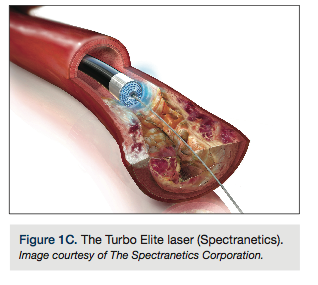 However, now we are seeing some of the sequelae of putting in stents, especially several stents. Patients can come back with recurrent stenosis and occlusions, and physicians are considering what other options are available besides putting in multiple stents.
However, now we are seeing some of the sequelae of putting in stents, especially several stents. Patients can come back with recurrent stenosis and occlusions, and physicians are considering what other options are available besides putting in multiple stents.
What are the different atherectomy devices?
In our presentation, we discussed:
- The SilverHawk/TurboHawk (Covidien), a directional atherectomy device;
- The Jetstream (Bayer Healthcare), a rotational atherectomy device;
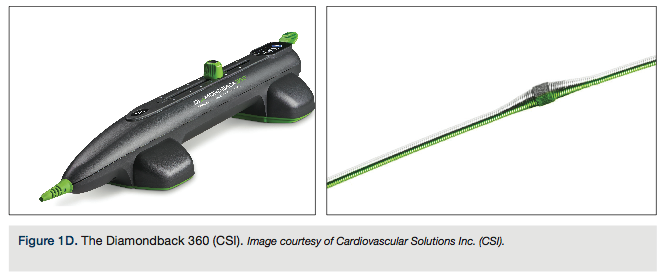
- The Diamondback 360˚ (CSI), an orbital atherectomy device;
- The Turbo Elite laser (Spectranetics), a photoablative device.

Can you give a best-case scenario for the use of each device?
For an eccentric lesion that contains anything from mild to severe calcification, then a directional atherectomy device (SilverHawk/TurboHawk) has a distinct advantage. If the lesion involves thrombus, the laser has a very distinct advantage for treatment. For below the knee, the laser device and the directional atherectomy device have distinct advantages. The presence of soft plaque really negates the use of the CSI Diamondback device, but for highly calcific, especially focal plaque, the Diamondback seems to have a distinct advantage over the other technologies. For in-stent restenosis with potential thrombus involvement, and above and below the knee popliteal combined disease, then the Jetstream rotational atherectomy device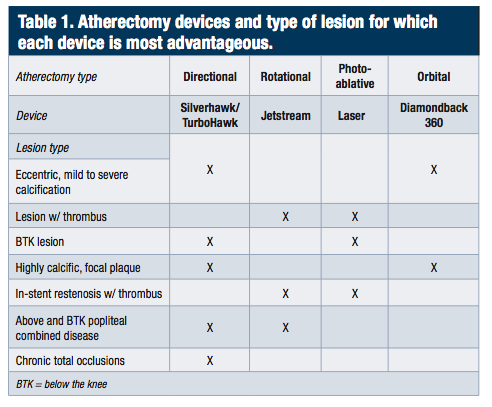 has an advantage, both in the cost savings of only using one device, as well as in the ability to aspirate thrombus and cut the atheroma itself. The Jetstream also has the advantage of two different cutting settings. The lower profile cutting can be used going down, especially below the knee, and then the higher, blades up setting allows you to achieve at least a 3.4-3.6 mm lumen. There are multiple indications for these different devices. None really has the whole market. Each one has a specific advantage and some disadvantages.
has an advantage, both in the cost savings of only using one device, as well as in the ability to aspirate thrombus and cut the atheroma itself. The Jetstream also has the advantage of two different cutting settings. The lower profile cutting can be used going down, especially below the knee, and then the higher, blades up setting allows you to achieve at least a 3.4-3.6 mm lumen. There are multiple indications for these different devices. None really has the whole market. Each one has a specific advantage and some disadvantages.
What about your own practice?
The majority of what I do is with a directional atherectomy device, because I deal with a lot of chronic total occlusions (CTOs).3 Directional atherectomy gives you the opportunity to cut towards the blockage, the atheroma, and not cut towards the wall itself, thus decreasing the risk of perforation. The directional atherectomy device is my workhorse catheter for CTOs. It allows us to cut calcium, and cut through both soft and moderate plaque, although directional atherectomy does not do well with thrombus or highly calcific, long lesions.
What is the learning curve for the use of atherectomy?
It is fairly straightforward. The basic theory of use behind any of these technologies is to go slow and let the device do the work. That is really true for all of the devices. Pushing to go faster with these devices means they are going to dotter and push through the plaque, and that leads to a higher likelihood of breaking a piece off as an embolus, or jumping through and not adequately cutting through the lesion. Accept the need to go slow and allow the cutter, whatever type of cutter it is, to do the work, and you will achieve very good results.
What about embolization?
The DEFINITIVE LE study4 looked at 800 patients, with over 1,000 lesions treated, and only about 1.6% of the patients in the study actually had an embolus requiring intervention, whether aspiration or something else. Only .1% required surgical intervention, so a surgery was extremely rare.
There are certain techniques that mandate the use of an embolic protection device. A calcium-cutting device that chips through plaque definitely requires the use of an embolic protection device. I tend to use an embolic protection device when I am dealing with fresh thrombus. Some operators say they use embolic protection for all their cases. That is another way of doing it; it just adds to the expense of the procedure.
Any final thoughts?
We are now seeing a greater acceptance of the use of atherectomy; people are realizing that it is not just for a few isolated cases. The management of the diabetic patient with peripheral arterial disease has always been challenging, with expected lower patencies than with the treatment of non-diabetic patients, regardless of the treatment modality, either surgical or endovascular. The DEFINITIVE LE study prospectively confirmed that there was no difference in one-year patency in diabetics versus non-diabetics. In the future, the real question will be: if debulking is paired with an atherectomy device, and an antiproliferative drug administered via a drug-coated balloon, can the incidence of restenosis be significantly decreased? When it is just the plaque, we still have to worry about the penetration of the drug, but if the plaque is debulked before the use of a drug-coated balloon, it may result in a significant decrease in restenosis. Some preliminary work was presented at VEITHSymposium, looking at the combination of anti-restenosis therapy in conjunction with atherectomy and showing an advantage, at least in the short term. That study is now being carried out over a longer period to determine the long-term impact.5
Disclosure: Dr. McKinsey reports he is the co-global PI of the DEFINITIVE LE study, co-national PI of the Phoenix trial; on the speakers panel for Covidien, Bayer, and Abbott; and on the scientific advisory board for Spectranetics Corporation.
Dr. James McKinsey can be contacted at jfm2111@columbia.edu.
References and recommended reading
- Lawrence A. Garcia, DEFINITIVE LE 12-Month Final Results [abstract]. VIVA 2012; Oct 9-12, 2012; Las Vegas, NV.
- McKinsey JF, Goldstein L, Khan HU, Graham A, Rezeyat C, Morrissey NJ, Sambol E, Kent KC. Novel Treatment of patients with lower extremity ischemia: use of percutaneous atherectomy in 579 lesions. Ann Surg. 2008 Oct; 248(4): 519-528.
- Gallagher KA, Meltzer AJ, Ravin RA, Graham A, Shrikhande G, Connolly PH, Aiello F, Dayal R, McKinsey JF. Endovascular management as first therapy for chronic total occlusion of the lower extremity arteries: comparison of balloon angioplasty, stenting, and directional atherectomy. J Endovasc Ther. 2011 Oct; 18(5): 624-637. doi: 10.1583/11-3539.1.
- DEFINITIVE LE: Study of SilverHawk/TurboHawk in Lower Extremity Vessels. Available online at https://www.turbohawkdevice.com/definitivele. Accessed December 11, 2013.
- Thomas Zeller, DEFINITIVE AR Acute Outcomes [abstract]. VIVA 2013; Oct 8-11, 2013; Las Vegas, NV.
- Khan SZ, Kahn MA, Connolly P, Gallagher K, Morrissey NJ, McKinsey JF. Endovascular tibial interventions in diabetic patients with critical limb ischemia (CLI): the role of atherectomy. Transcather Cardiovascular Therapeutics, September 2010.
