


The Utility of Fractional Flow Reserve Post-Coronary Artery Bypass Grafting
Abstract
Fractional flow reserve (FFR) has been validated as a useful tool in the physiological assessment of coronary artery lesions. However, the utility of FFR in saphenous vein graft lesions has not been extensively evaluated. Herein, we present a case with dual compromised flow from the native circulation and a bypass graft, which was found to be suboptimal using FFR of the distal myocardial segment.
assessment of coronary artery lesions. However, the utility of FFR in saphenous vein graft lesions has not been extensively evaluated. Herein, we present a case with dual compromised flow from the native circulation and a bypass graft, which was found to be suboptimal using FFR of the distal myocardial segment.
Case
A 70-year-old male with medical history of ischemic heart disease status post remote coronary artery bypass graft surgery, calcific aortic valve stenosis status post mechanical aortic valve replacement, atrial fibrillation, and chronic systolic heart failure with left ventricular systolic ejection fraction of 20%, presented after acute onset of chest discomfort followed by a single discharge from his previously implanted defibrillator. Interrogation of the device confirmed an appropriate shock for ventricular tachycardia after a failed attempt of anti-tachycardia pacing. Subsequently, the patient was referred for coronary and graft angiography to rule out progression of coronary artery disease.
Coronary angiography revealed severe native disease involving a mid left circumflex artery 70-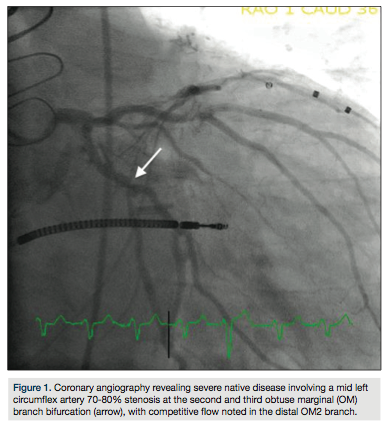 80% stenosis at the second and third obtuse marginal (OM) branch bifurcation, with competitive flow noted in the distal OM2 branch (Figure 1). Selective graft angiography of the left internal mammary artery (LIMA) to the mid left anterior descending artery demonstrated a patent jump graft from LIMA to OM2 with a distal anastamotic 60-70% stenosis (Figure 2). Due to concern for the adequacy of perfusion of the OM2 segment via the native circulation or the jump graft, a strategy to measure the fractional flow reserve (FFR) in the distal OM2 branch was pursued. After maximal hyperemia using intravenous adenosine infusion at 180 mcg/kg/min, maximal FFR was calculated at 0.80 (Figure 3a) with a PressureWire (St. Jude
80% stenosis at the second and third obtuse marginal (OM) branch bifurcation, with competitive flow noted in the distal OM2 branch (Figure 1). Selective graft angiography of the left internal mammary artery (LIMA) to the mid left anterior descending artery demonstrated a patent jump graft from LIMA to OM2 with a distal anastamotic 60-70% stenosis (Figure 2). Due to concern for the adequacy of perfusion of the OM2 segment via the native circulation or the jump graft, a strategy to measure the fractional flow reserve (FFR) in the distal OM2 branch was pursued. After maximal hyperemia using intravenous adenosine infusion at 180 mcg/kg/min, maximal FFR was calculated at 0.80 (Figure 3a) with a PressureWire (St. Jude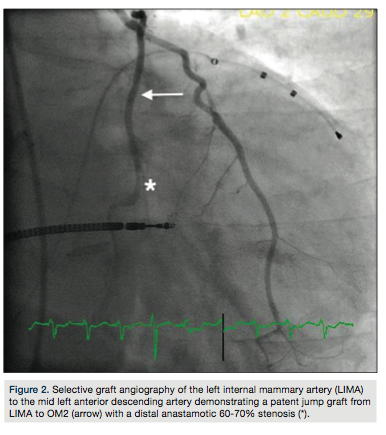 Medical) in the OM2 segment distal to the graft anastamosis (Figure 3b). A pullback FFR revealed a maximal value at 0.75 (Figure 4a) with the PressureWire wire in the OM2 segment proximal to the graft anastamosis (Figure 4b). Due to the suggestion of borderline perfusion in the distal OM2 segment despite the bypass graft, percutaneous coronary intervention (PCI) of the mid left circumflex artery was performed using a Veriflex 3.0 x 16 mm bare metal stent (Boston Scientific) with excellent angiographic result and brisk retrograde flow through the bypass graft (Figure 5).
Medical) in the OM2 segment distal to the graft anastamosis (Figure 3b). A pullback FFR revealed a maximal value at 0.75 (Figure 4a) with the PressureWire wire in the OM2 segment proximal to the graft anastamosis (Figure 4b). Due to the suggestion of borderline perfusion in the distal OM2 segment despite the bypass graft, percutaneous coronary intervention (PCI) of the mid left circumflex artery was performed using a Veriflex 3.0 x 16 mm bare metal stent (Boston Scientific) with excellent angiographic result and brisk retrograde flow through the bypass graft (Figure 5).
Discussion
FFR is derived from the ratio of the mean distal coronary-artery pressure to the aortic pressure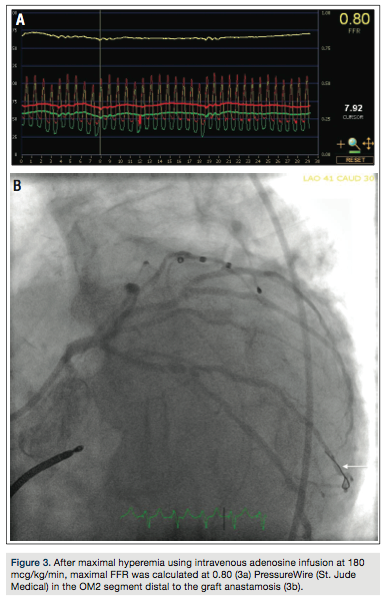 during maximal vasodilation, and was first reliably demonstrated as a technique to determine functionally significant coronary stenoses by Pijls et al in 1996.1 Since then, additional studies have corroborated the advantages of FFR to determine the physiologic significance of anatomic lesions in the coronary vasculature. The DEFER trial demonstrated that the deferral of PCI based on an FFR > 0.75 led to no difference in outcomes, carried out to five years.2 The FAME study concluded that routine measurement of FFR in patients with multi-vessel coronary artery disease undergoing PCI significantly reduces major adverse cardiac events at one year.3 These data on the validity of FFR for physiological assessment of coronary lesions led
during maximal vasodilation, and was first reliably demonstrated as a technique to determine functionally significant coronary stenoses by Pijls et al in 1996.1 Since then, additional studies have corroborated the advantages of FFR to determine the physiologic significance of anatomic lesions in the coronary vasculature. The DEFER trial demonstrated that the deferral of PCI based on an FFR > 0.75 led to no difference in outcomes, carried out to five years.2 The FAME study concluded that routine measurement of FFR in patients with multi-vessel coronary artery disease undergoing PCI significantly reduces major adverse cardiac events at one year.3 These data on the validity of FFR for physiological assessment of coronary lesions led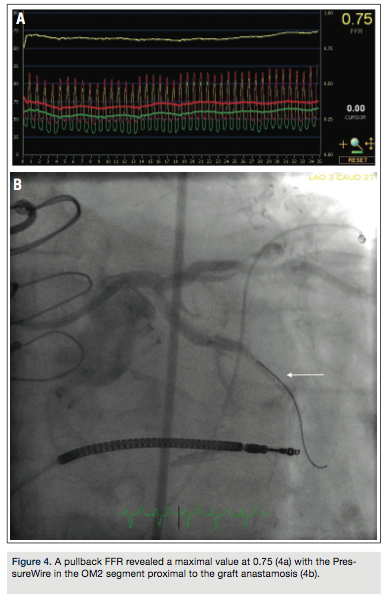 to the American Heart Association (AHA) scientific statement on FFR’s use in improving patient care.4
to the American Heart Association (AHA) scientific statement on FFR’s use in improving patient care.4
The use of FFR in bypass vein grafts, however, has not been extensively evaluated. In one small study, 10 patients with saphenous vein graft lesions and corresponding myocardial perfusion imaging (MPI) studies were evaluated to determine the accuracy of FFR.5 The use of FFR to assess the physiological significance of SVG lesions was found to be feasible, with acceptable specificity and negative predictive value compared to stress MPI, using an FFR cutoff value of 0.75. Meanwhile, several studies have validated the predictability of graft patency using FFR. Botman et al, in a study of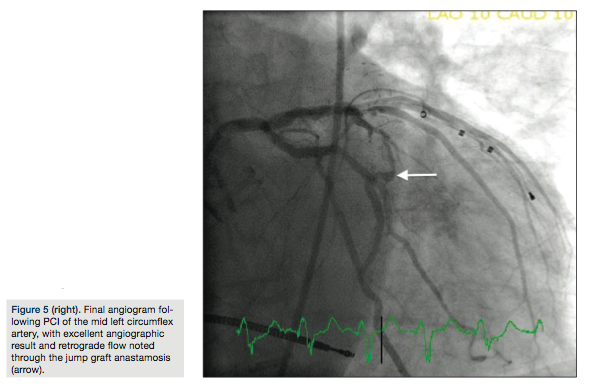 164 patients, demonstrated that the patency of bypass grafts on functionally significant lesions is significantly higher than the patency of bypass grafts on non-significant lesions.6
164 patients, demonstrated that the patency of bypass grafts on functionally significant lesions is significantly higher than the patency of bypass grafts on non-significant lesions.6
The additional utility of FFR in patients with bypass grafts, as shown in the case presented here, is to assess the physiological significance of lesions when the distal myocardium is perfused by compromised flow from an epicardial vessel along with an alternate compromised source, including a bypass graft with a lesion or a suboptimal collateral vessel. In these cases, FFR can be derived separately for the myocardium that takes into consideration maximal flow into the specific myocardial segment via all available channels. Thereby, if the FFR wire is placed distal to the bypass graft anastamosis or the collateral channel, the FFR calculated at maximal hyperemia reflects the myocardial perfusion pressure, including the flow via the native and collateral circulations.
We present herein a case of dual compromised flow from the native circulation and a bypass graft, which was found to be suboptimal using FFR of the distal myocardial segment, thereby prompting PCI after demonstration of physiologic significance of the lesions.
Disclosure: Dr. George reports that he is a consultant for Boston Scientific.
Jon C. George, MD, can be contacted at jcgeorgemd@gmail.com.
References
- Pijls NHJ, de Bruyne B, Peels K, et al. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med. 1996; 334: 1703-1708.
- Pijls NHJ, van Schaardenburgh P, Manoharan G, et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5 year follow-up of the DEFER study. J Am Coll Cardiol. 2007; 49: 2105-2111.
- Tonino PAL, de Bruyne B, Pijls NHJ, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary interventions. N Engl J Med. 2009; 360: 213-224.
- Kern MJ, Lerman A, Bech JW, et al. Physiological assessment of coronary artery disease in the cardiac catheterization laboratory. A scientific statement from the American Heart Association Committee on Diagnostic and Interventional Cardiac Catheterization, Council on Clinical Cardiology. Circulation. 2006; 114: 1321-1341.
- Aqel R, Zoghbi GJ, Hage F, et al. Hemodynamic evaluation of coronary artery bypass graft lesions using fractional flow reserve. Cathet Cardiovasc Interv. 2008; 72: 479-485.
- Botman CJ, Schonberger J, Koolen S, et al. Does stenosis severity of native vessels influence bypass graft patency? A prospective fractional flow reserve-guided study. Ann Thorac Surg. 2007; 83: 2093-2097.
