


Use of a Coronary Wire for Temporary Pacing
Mr. DO is 54-year-old gentleman who presented to our emergency room with acute onset of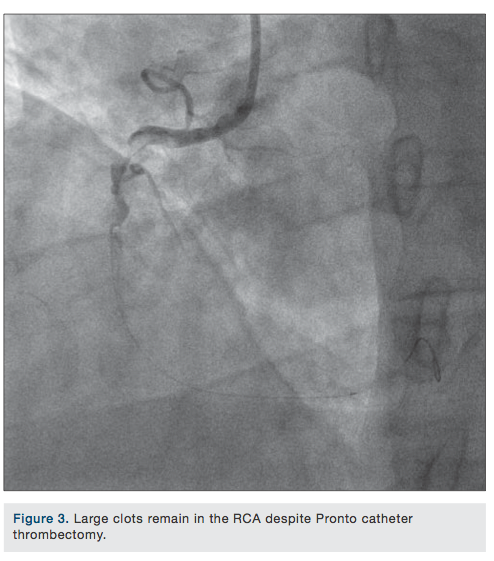 chest pain. An electrocardiogram performed in the emergency room showed nonspecific ST-T changes. The patient received aspirin, heparin, and ticagrelor (Brilinta, AstraZeneca) before he was taken to the cardiac catheterization laboratory. Eptifibatide (Integrilin, Millennium Pharmaceuticals/Schering-Plough) was given as double bolus, followed by a drip.
chest pain. An electrocardiogram performed in the emergency room showed nonspecific ST-T changes. The patient received aspirin, heparin, and ticagrelor (Brilinta, AstraZeneca) before he was taken to the cardiac catheterization laboratory. Eptifibatide (Integrilin, Millennium Pharmaceuticals/Schering-Plough) was given as double bolus, followed by a drip.
Coronary angiography revealed evidence of severe disease involving the left anterior descending coronary artery (LAD) and the circumflex artery. Right coronary angiography showed a totally occluded right coronary artery filled with a large thrombus (Figure 1). The right coronary artery was successfully cannulated with 0.14 Balance Middleweight (BMW) universal wire (Abbott Vascular) (Figure 2). An unsuccessful attempt was made to perform thrombectomy in the right coronary artery using a Pronto V3 extraction catheter (Vascular Solutions) (Figure 3). At this point, an AngioJet (Medrad/Bayer HealthCare) was inserted and advanced into the right coronary artery to perform thrombectomy, in view of the large size of the thrombus (Figure 4). The distal end of the coronary wire was hooked up with the negative port of the pacemaker generator. The positive port was clipped to the patient’s skin for grounding. As expected, during the AngioJet procedure, the patient went into complete heart block and the pacemaker wire successfully paced from the right coronary artery as shown in Figure 5. Following the successful thrombectomy, two Xience stents (Abbott Vascular), 3.5 x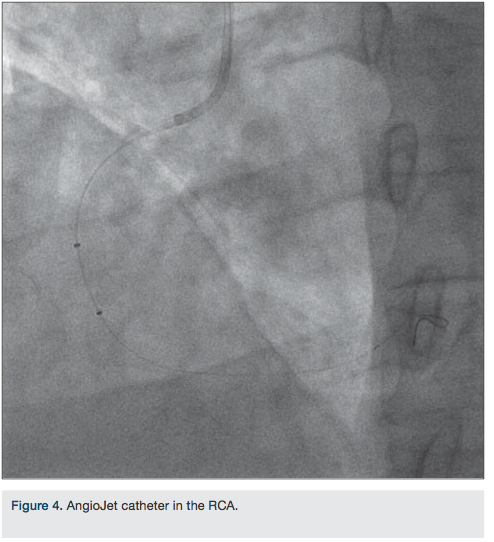 18 mm and 3.5 x 8 mm, were successfully deployed. TIMI-III flow was achieved (Figure 6). The patient’s condition was stable and he was pacing on his own with normal sinus rhythm. The patient’s chest pain and ST elevation had disappeared, and he was taken back to the coronary care unit in stable condition.
18 mm and 3.5 x 8 mm, were successfully deployed. TIMI-III flow was achieved (Figure 6). The patient’s condition was stable and he was pacing on his own with normal sinus rhythm. The patient’s chest pain and ST elevation had disappeared, and he was taken back to the coronary care unit in stable condition.
This case illustrates the benefits of using the angioplasty coronary wire as means for pacing the right ventricle without necessarily requiring a temporary pacemaker insertion into the right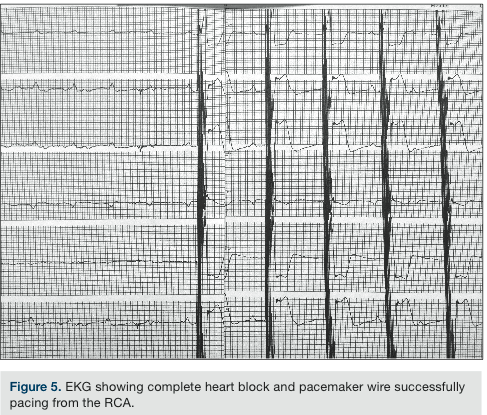 ventricle. At our facility, a transvenous temporary pacemaker is only rarely used for temporary pacing. It is important, however, to check for pacemaker sensitivity and capture prior using the AngioJet.
ventricle. At our facility, a transvenous temporary pacemaker is only rarely used for temporary pacing. It is important, however, to check for pacemaker sensitivity and capture prior using the AngioJet.
Disclosure: Dr. Dabbous reports no conflicts of interest regarding the content herein.
Samir Dabbous, MD, can be contacted at sdabbous@gmail.com
