


Unusual Form of a Supracardiac Type Total Anomalous Pulmonary Venous Connection
Abstract
Most patients with a total anomalous pulmonary venous connection have a set pattern of pulmonary venous drainage and predictable sites of obstruction. However, uncommon variations do exist and delineating the entire course is more important than just knowing the site of drainage. This report describes a newborn girl with an unusual form of the supracardiac type of total anomalous pulmonary venous connection, where all pulmonary veins drained into the right-sided systemic veins with a common inlet left ventricle.
Introduction
A total anomalous pulmonary venous connection develops when the primordial pulmonary veins fail to unite with the plexus of veins surrounding the lung buds. Four types have been identified:
- Type 1, anomalous connection at the supracardiac level;
- Type 2, anomalous connection at the cardiac level;
- Type 3, anomalous connection at the infracardiac level; and
- Type 4, anomalous connection at two or more of the above levels.1
The supracardiac type is the most common form of diagnosed total anomalous pulmonary venous connection.2 These congenital heart anomalies can be associated with heterotaxy syndrome.3 In the case herein, a newborn girl was discovered to possess an unusual form of the supracardiac type of total anomalous pulmonary venous connection, associated with complex cardiac anomalies instead of heterotaxy syndrome.
Case report
A 15-day-old female newborn with moderate cyanosis was referred to our department for cardiac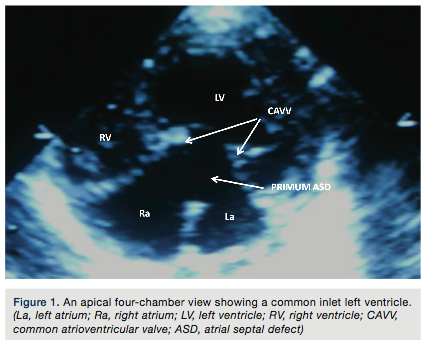 evaluation. On initial examination, the lips and tongue were blue, and ejection systolic murmur was heard all over the precordium. Oxygen saturation was 85% in the room air. The electrocardiogram showed left axis deviation and chest X-ray revealed cardiomegaly with pulmonary plethora. The echocardiography showed a common inlet left ventricle with ventricular septal defect and normally related great arteries (Figure 1). The subcostal view revealed that the pulmonary veins connected to a systemic vein (Figure 2a-b). Abdominal ultrasonography revealed a normally located liver and spleen. A cardiac catheterization was performed for further evaluation and showed that the right pulmonary veins were opening into the region of the superior vena cava and right atrium junction (Figure 3a, supplementary video 1). In addition, the left upper and lower pulmonary veins were forming a long, common systemic vein that was opening into the superior vena cava (Figure 3b, supplementary video 2). After
evaluation. On initial examination, the lips and tongue were blue, and ejection systolic murmur was heard all over the precordium. Oxygen saturation was 85% in the room air. The electrocardiogram showed left axis deviation and chest X-ray revealed cardiomegaly with pulmonary plethora. The echocardiography showed a common inlet left ventricle with ventricular septal defect and normally related great arteries (Figure 1). The subcostal view revealed that the pulmonary veins connected to a systemic vein (Figure 2a-b). Abdominal ultrasonography revealed a normally located liver and spleen. A cardiac catheterization was performed for further evaluation and showed that the right pulmonary veins were opening into the region of the superior vena cava and right atrium junction (Figure 3a, supplementary video 1). In addition, the left upper and lower pulmonary veins were forming a long, common systemic vein that was opening into the superior vena cava (Figure 3b, supplementary video 2). After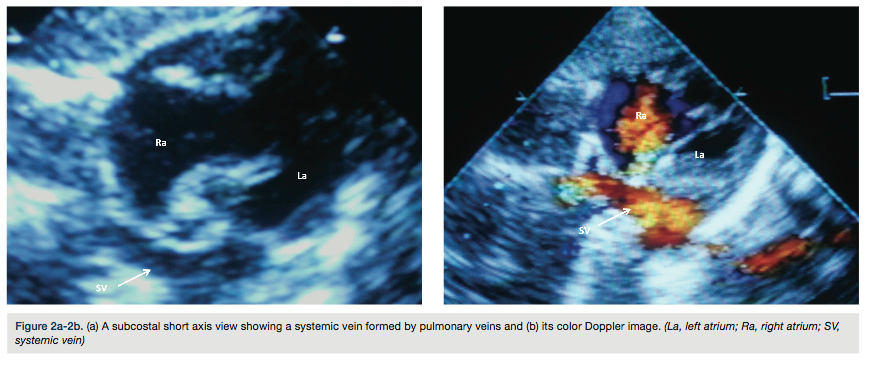 discussion with the child’s parents, who were made aware of the high risk of a surgical procedure, the patient referred for cardiac surgery with a median sternotomy approach. The right atrium and superior vena cava were grossly dilated. The right upper and lower pulmonary veins were opening into the superior vena cava just above the orifice of the right atrium. On the other hand, all the left pulmonary veins were opening into superior vena cava with a long, common, right-sided systemic vein. The pulmonary venous confluence was attached to the left atrium via a 2 cm incision. However, the patient expired post-operatively due ventricular arrhythmias.
discussion with the child’s parents, who were made aware of the high risk of a surgical procedure, the patient referred for cardiac surgery with a median sternotomy approach. The right atrium and superior vena cava were grossly dilated. The right upper and lower pulmonary veins were opening into the superior vena cava just above the orifice of the right atrium. On the other hand, all the left pulmonary veins were opening into superior vena cava with a long, common, right-sided systemic vein. The pulmonary venous confluence was attached to the left atrium via a 2 cm incision. However, the patient expired post-operatively due ventricular arrhythmias.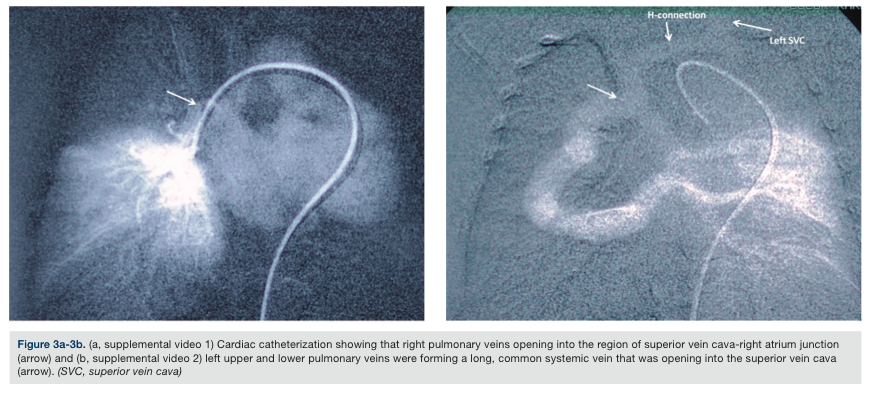
Discussion
Total anomalous pulmonary venous connection is a rare congenital anomaly, corresponding to approximately 2% of all congenital heart defects.1,2 It consists of an abnormality of blood flow in which all four pulmonary veins drain into systemic veins or the right atrium, with or without pulmonary venous obstruction. Total pulmonary venous connection and its unusual forms are well recognized in complex cardiac defects and heterotaxy syndrome.3 In our case, the common inlet left ventricle was the complex cardiac defect, without any heterotaxy syndrome. Total anomalous pulmonary venous connection is a rare congenital anomaly in which echocardiography is sufficient for diagnosis. Apical, four-chamber and subcostal echocardiographic views can best identify individual pulmonary veins and their confluence. However, cardiac catheterization should be considered as one of the several complementary imaging modalities to show delineated anatomy, drainage, and obstruction of all four pulmonary veins. The correct preoperative diagnosis and an accurate anatomic description are essential for planning surgical treatment of these patients. In the patient’s unusual form of supracardiac type total anomalous pulmonary venous connection, all pulmonary veins drained into the right-sided systemic veins.
Disclosure: The authors report no financial relationships or conflict of interest regarding the content herein.
The authors can be contacted via Dr. Hayrullah Alp at drhayrullahalp@hotmail.com.
References
- Bharati S, Lev M. Congenital anomalies of the pulmonary veins. Cardiovasc Clin. 1973; 5(1): 23-41.
- Geva T, van Praagh S. Anomalies of the pulmonary veins. In: Allen H, Driscoll D, Shaddy R, Feltes T (eds). Moss and Adams’ heart disease in infants, children, and adolescents. Vol 2. 7th ed. Philadelphia, Pennsylvania: Lippincott Williams & Wilkins, 2008: 761-791.
- Lehner A, Kozlik-Feldmann R, Herrmann F, et al. An unusual form of supracardiac total anomalous pulmonary venous return via a right-sided vertical vein in a heterotaxy syndrome case. Pediatr Cardiol 2012; 33(7): 1200-1202.
______________________________
*Research Fellow, Necmettin Erbakan University, Meram School of Medicine Hospital, Department of Pediatric Cardiology, Konya, Turkey; †Professor, Necmettin Erbakan University, Meram School of Medicine Hospital, Department of Pediatric Cardiology, Konya, Turkey
