


Treatment of a Heavily Calcified SFA Utilizing the Jetstream Navitus L
Case report
Procedural indication: Rutherford Class III activity-limiting claudication in a 74-year-old male with established peripheral arterial disease and diabetes mellitus type 2.
The patient was brought to the cardiac catheterization lab in a fasting state, and prepped and draped in a sterile fashion. The left common femoral region was anesthetized via 20 mL of 2% lidocaine. The left common femoral artery was accessed under ultrasound guidance using a micropuncture kit and a 5 French arterial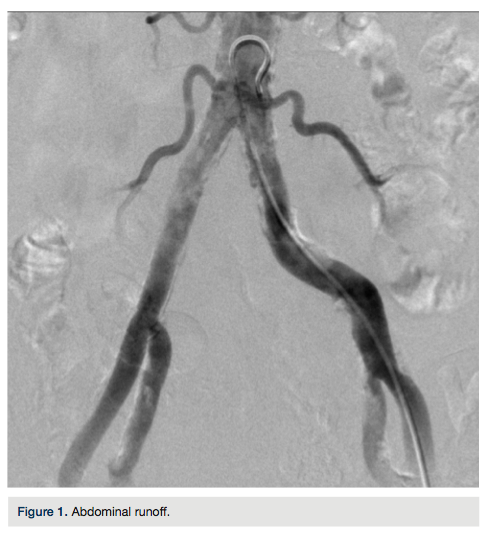 sheath was advanced over the wire using modified Seldinger technique. Next, a Contra catheter (Boston Scientific) was advanced into the abdominal aorta. Abdominal aortography was performed, demonstrating a 40% to 50% mid left common femoral arterial stenosis (Figure 1); however, it was not found to be hemodynamically significant. The catheter was advanced over a wire to the proximal right superficial femoral artery. Angiographic images performed in oblique as well as anteroposterior (AP) projections demonstrated an 80% to 90% distal right
sheath was advanced over the wire using modified Seldinger technique. Next, a Contra catheter (Boston Scientific) was advanced into the abdominal aorta. Abdominal aortography was performed, demonstrating a 40% to 50% mid left common femoral arterial stenosis (Figure 1); however, it was not found to be hemodynamically significant. The catheter was advanced over a wire to the proximal right superficial femoral artery. Angiographic images performed in oblique as well as anteroposterior (AP) projections demonstrated an 80% to 90% distal right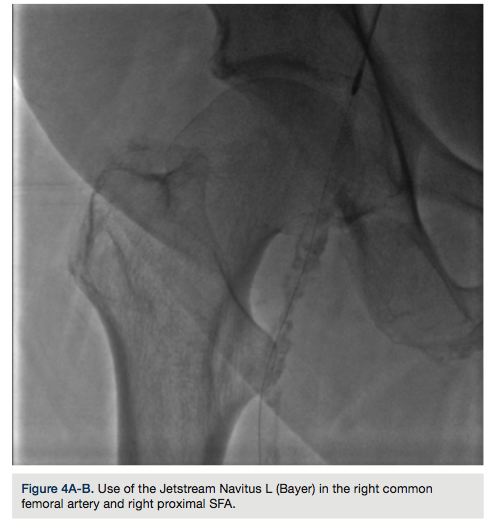 common femoral arterial stenosis that was heavily calcified, extending to the proximal right superficial femoral artery (Figure 2). In addition, another sequential 80% to 90% mid right superficial femoral artery stenosis existed above the level of Hunter’s canal (Figure 3). The decision was made to proceed with revascularization. A Glidewire Advantage (Terumo) was advanced into the popliteal artery. The 5 French sheath and the Contra catheter were withdrawn. Advancement of a 7 French Destination sheath (Terumo) was attempted across the aortic bifurcation; however, due to the left common femoral arterial severe
common femoral arterial stenosis that was heavily calcified, extending to the proximal right superficial femoral artery (Figure 2). In addition, another sequential 80% to 90% mid right superficial femoral artery stenosis existed above the level of Hunter’s canal (Figure 3). The decision was made to proceed with revascularization. A Glidewire Advantage (Terumo) was advanced into the popliteal artery. The 5 French sheath and the Contra catheter were withdrawn. Advancement of a 7 French Destination sheath (Terumo) was attempted across the aortic bifurcation; however, due to the left common femoral arterial severe calcification, this was unsuccessful. The dilator was withdrawn from the sheath and a Quick-Cross catheter (Spectranetics) was advanced into the popliteal artery. The Glidewire was withdrawn and a Supra Core wire (Abbott Vascular) was advanced in the popliteal artery. This time, the dilator was advanced again over the Supra Core wire, and with some difficulty, the sheath was advanced to the level of the distal right external iliac artery. Over the Supra Core wire, the Quick-Cross catheter was withdrawn and 7000 units of unfractionated heparin
calcification, this was unsuccessful. The dilator was withdrawn from the sheath and a Quick-Cross catheter (Spectranetics) was advanced into the popliteal artery. The Glidewire was withdrawn and a Supra Core wire (Abbott Vascular) was advanced in the popliteal artery. This time, the dilator was advanced again over the Supra Core wire, and with some difficulty, the sheath was advanced to the level of the distal right external iliac artery. Over the Supra Core wire, the Quick-Cross catheter was withdrawn and 7000 units of unfractionated heparin administered for dose and schedule. A Jetstream Navitus L (Bayer Healthcare) atherectomy catheter was used to perform atherectomy with blades down, as well as blades up, to the right common femoral artery and proximal right superficial artery (Figure 4A). The catheter was also used to perform atherectomy of the mid right superficial femoral artery with blades down, as well as blades up (Figure 4B). The device was withdrawn. Significant luminal gain was appreciated angiographically. At this point, a 6.0 x 100 mm AngioSculpt balloon (AngioScore) was advanced over the wire and used to perform balloon angioplasty to
administered for dose and schedule. A Jetstream Navitus L (Bayer Healthcare) atherectomy catheter was used to perform atherectomy with blades down, as well as blades up, to the right common femoral artery and proximal right superficial artery (Figure 4A). The catheter was also used to perform atherectomy of the mid right superficial femoral artery with blades down, as well as blades up (Figure 4B). The device was withdrawn. Significant luminal gain was appreciated angiographically. At this point, a 6.0 x 100 mm AngioSculpt balloon (AngioScore) was advanced over the wire and used to perform balloon angioplasty to the mid distal right common femoral artery, extending to the proximal right superficial femoral artery. The balloon was inflated to 10 atmospheres for 1 minute, deflated, and withdrawn. Repeat angiographic images demonstrated excellent procedural results, with less than 20% residual stenosis and brisk two-vessel runoff to the right foot (Figure 5). There was no evidence of embolic complications. At this point, the procedure was considered concluded. The wire was withdrawn. The sheath was withdrawn over a wire after re-cleansing the groin with
the mid distal right common femoral artery, extending to the proximal right superficial femoral artery. The balloon was inflated to 10 atmospheres for 1 minute, deflated, and withdrawn. Repeat angiographic images demonstrated excellent procedural results, with less than 20% residual stenosis and brisk two-vessel runoff to the right foot (Figure 5). There was no evidence of embolic complications. At this point, the procedure was considered concluded. The wire was withdrawn. The sheath was withdrawn over a wire after re-cleansing the groin with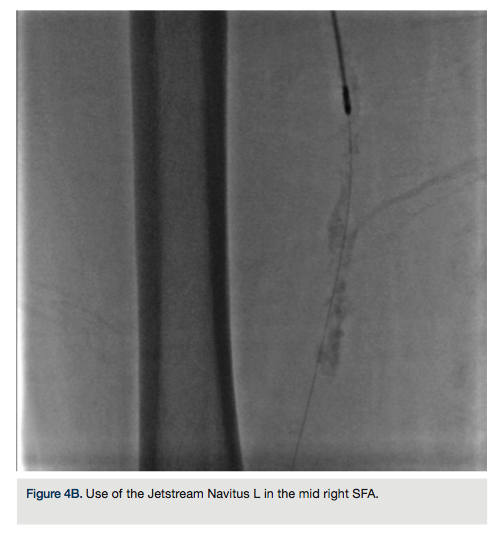 chlorhexidine, and a Perclose vascular closure (Abbott Vascular) device was used to obtain hemostasis. The patient was subsequently transferred to the cardiovascular recovery area for further observation and care, with plans for continuation of aspirin and clopidogrel dual-antiplatelet therapy.
chlorhexidine, and a Perclose vascular closure (Abbott Vascular) device was used to obtain hemostasis. The patient was subsequently transferred to the cardiovascular recovery area for further observation and care, with plans for continuation of aspirin and clopidogrel dual-antiplatelet therapy.
Disclosure: Orlando Marrero reports he is an endovascular consultant for Bayer Interventional. Dr. Amit Srivastava reports no conflicts of interest regarding the content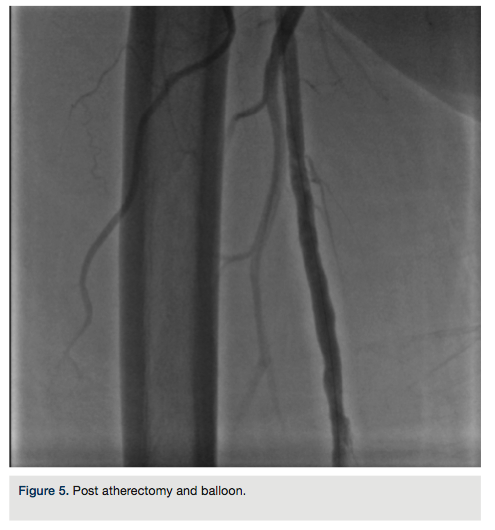 herein.
herein.
Orlando Marrero can be contacted at orlm8597@yahoo.com
