


Transradial Szabo Technique
![]()
A 64-year-old female with history of coronary artery disease, previous stent of the ostial right coronary artery (RCA) and a previous mid RCA stent, presented with unstable angina symptoms. She underwent diagnostic angiography via the right radial artery with K. S. Chandrasekhar, MD. A 90% in-stent ostial restenosis of the RCA was found (Figure 1), as well as incomplete ostial coverage with the prior stent. The patient was referred for revascularization.
 Procedure
Procedure
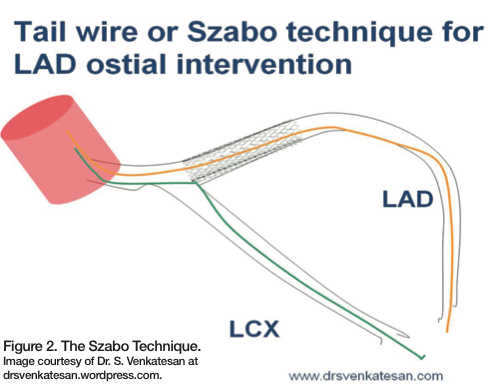
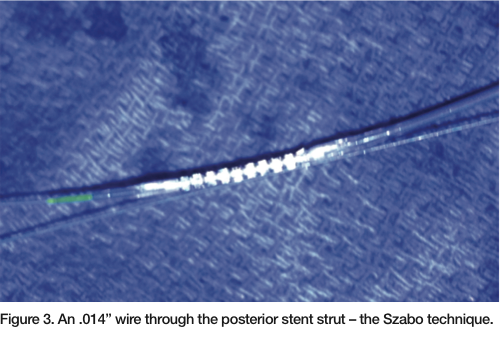
The right radial artery was upsized to a 6 French Glidesheath (Terumo). An Amplatz right (AR) Mod guide catheter was modified with iatrogenic side holes. We then engaged the RCA system, advancing a Runthrough guide wire (Terumo) distally. A 0.9 mm laser catheter was used to perform laser atherectomy initially at 45/25 and then at 60/40 for two passes in the ostial RCA, reducing the stenosis from 90% to 50%. Predilation was performed with a 3.5 mm x 10 mm AngioSculpt scoring balloon (AngioScore) at 12 atm. A 3.5 x 12mm Promus drug-eluting stent (Boston Scientific) was placed 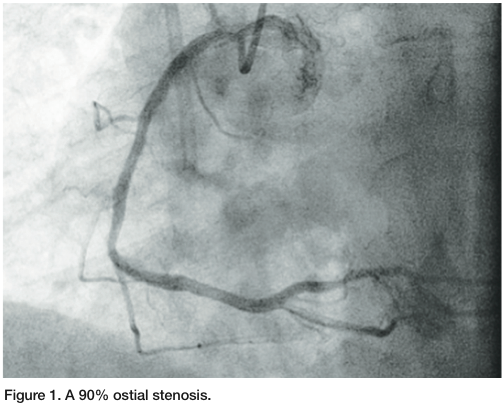 using the Szabo technique1 (Figures 2-3), with a second wire placed in the aortic root to ensure ostial placement (Figure 4). The stent was then advanced to the ostium, deployed, and then the second wire was removed from the proximal strut, ensuring that we were ostial in placement. We post-dilated with a 3.75mm Quantum balloon (Boston Scientific) at high pressure. Final angiography revealed TIMI-3 flow without any dissection, perforation, or embolization. The patient tolerated the procedure well.
using the Szabo technique1 (Figures 2-3), with a second wire placed in the aortic root to ensure ostial placement (Figure 4). The stent was then advanced to the ostium, deployed, and then the second wire was removed from the proximal strut, ensuring that we were ostial in placement. We post-dilated with a 3.75mm Quantum balloon (Boston Scientific) at high pressure. Final angiography revealed TIMI-3 flow without any dissection, perforation, or embolization. The patient tolerated the procedure well.
Discussion
 One of the primary objectives of treating ostial lesions is the correct placement of the stent to optimize lesion coverage and avoid geographic miss. Ostial lesions are associated with increased restenosis, even in the drug-eluting stent era.2 This is due in part to lesion rigidity, calcification and elastic recoil. Angiographic determination of accurate stent placement has limitations and various techniques, and devices have been proposed to facilitate accurate placement. The Szabo technique uses a second wire through a trailing strut to allow for accurate stent placement. This technique appears to obviate the limitations of angiographic placement and does not require any adjunctive devices.
One of the primary objectives of treating ostial lesions is the correct placement of the stent to optimize lesion coverage and avoid geographic miss. Ostial lesions are associated with increased restenosis, even in the drug-eluting stent era.2 This is due in part to lesion rigidity, calcification and elastic recoil. Angiographic determination of accurate stent placement has limitations and various techniques, and devices have been proposed to facilitate accurate placement. The Szabo technique uses a second wire through a trailing strut to allow for accurate stent placement. This technique appears to obviate the limitations of angiographic placement and does not require any adjunctive devices.
 The technique was first described by Szabo et al in 2005 and involves a second guide wire placed in the aorta (or branch vessel for a non aorto-ostial lesion) to anchor the stent.1 The stent is prepared by a low pressure inflation (1-2 atm) with the protective sleeve left in place while exposing the proximal struts. The remainder of the stent is compressed with the sleeve. The wire is passed through the proximal strut of the stent followed by crimping of the “lifted” strut; however, not to the degree that the anchor wire is not mobile. The stent then travels over the primary guide wire and the anchor wire, which stops forward motion of the stent at the
The technique was first described by Szabo et al in 2005 and involves a second guide wire placed in the aorta (or branch vessel for a non aorto-ostial lesion) to anchor the stent.1 The stent is prepared by a low pressure inflation (1-2 atm) with the protective sleeve left in place while exposing the proximal struts. The remainder of the stent is compressed with the sleeve. The wire is passed through the proximal strut of the stent followed by crimping of the “lifted” strut; however, not to the degree that the anchor wire is not mobile. The stent then travels over the primary guide wire and the anchor wire, which stops forward motion of the stent at the 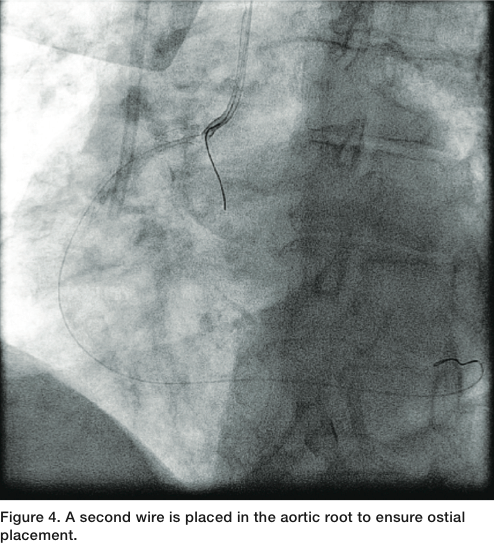 vessel ostium (Figures 2-3).3 The stent is then deployed at low or nominal pressure, followed by removal of the anchor wire. The stent balloon can then be reinflated or another balloon can be used to post dilate.
vessel ostium (Figures 2-3).3 The stent is then deployed at low or nominal pressure, followed by removal of the anchor wire. The stent balloon can then be reinflated or another balloon can be used to post dilate.
Caution must be used when applying this technique. Intravascular ultrasound follow-up has demonstrated stent protrusion and distortion, which may be more a concern in non aorto-ostial lesions. In addition, there is the potential for stent 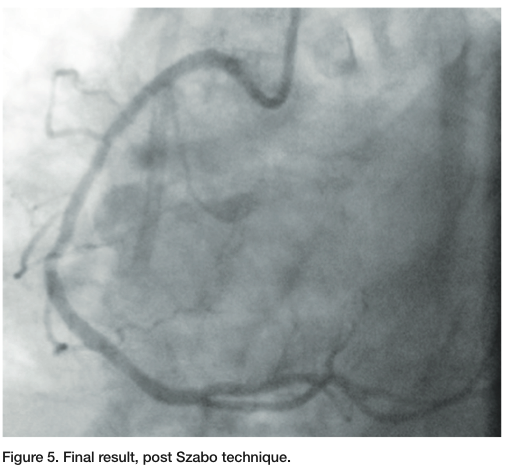 dislodgement as a result of stent manipulation. While the Szabo technique is not without limitations, it seems to provide complete ostial coverage for aorto-ostial lesions.4
dislodgement as a result of stent manipulation. While the Szabo technique is not without limitations, it seems to provide complete ostial coverage for aorto-ostial lesions.4
Orlando Marrero can be contacted at orlm8597@yahoo.com.
Dr. Zaheed Tai can be contacted at zaheedtai@gmail.com.
References
- Szabo S, Abramowitz B, Vaitkus PT. New technique for aorto-ostial stent placement. Am J Cardiol. 2005;96:212H.
- Mavromatis K, Ghazzal Z, Veledar E, Diamandopoulos L, Weintraub WS, Douglas JS, Kalynych AM. Comparison of outcomes of percutaneous coronary intervention of ostial versus nonostial narrowing of the major epicardial coronary arteries. Am J Cardiol. 2004;94:583-587.
- Kern MJ, Ouellette D, Frianeza T. A new technique to anchor stents for exact placement in ostial stenoses: The stent tail wire or Szabo technique. Catheter Cardiovasc Interv. 2006;68:901-906.
- Vaquerizo, et al. Bench top evaluation and clinical experience with the Szabo technique: new questions for a complex lesion. Catheter Cardiovasc Interv. 2012: 79:378-389.
