


Transradial Rotational Atherectomy and Kissing Balloon Technique
 Presentation
Presentation
The patient is a 63-year-old gentleman with diabetes who has been complaining of typical exertional angina-type chest discomfort and underwent diagnostic angiography earlier in the day. The patient demonstrated an 80 to 90% left anterior descending coronary artery (LAD) stenosis involving a moderate-size diagonal. He is referred to our lab for revascularization.
Procedure
 The patient was accessed through the right radial artery. The right radial artery sheath was exchanged under sterile technique for a 6 French Glidesheath (Terumo). Initially, a Q 3.5 guide wire (Boston Scientific) was used to engage the left coronary system. Bivalirudin (The Medicines Company) was administered. A Runthrough wire (Terumo) was passed distally into the left anterior descending coronary artery (LAD) as well as into the diagonal.
The patient was accessed through the right radial artery. The right radial artery sheath was exchanged under sterile technique for a 6 French Glidesheath (Terumo). Initially, a Q 3.5 guide wire (Boston Scientific) was used to engage the left coronary system. Bivalirudin (The Medicines Company) was administered. A Runthrough wire (Terumo) was passed distally into the left anterior descending coronary artery (LAD) as well as into the diagonal.
We  then attempted to advance the 2.5 x 15mm AngioSculpt scoring balloon (AngioScore), but were unsuccessful. An EBU 3.5 guiding catheter (Medtronic) was inserted after the wire was removed, the vessel was re-wired with a Runthrough wire, and we were still unsuccessful in passing the AngioSculpt balloon. We then sent a 1.25 over-the-wire balloon over the Runthrough, advanced a second Runthrough wire distally, and changed out for a floppy RotaWire (Boston Scientific).
then attempted to advance the 2.5 x 15mm AngioSculpt scoring balloon (AngioScore), but were unsuccessful. An EBU 3.5 guiding catheter (Medtronic) was inserted after the wire was removed, the vessel was re-wired with a Runthrough wire, and we were still unsuccessful in passing the AngioSculpt balloon. We then sent a 1.25 over-the-wire balloon over the Runthrough, advanced a second Runthrough wire distally, and changed out for a floppy RotaWire (Boston Scientific).
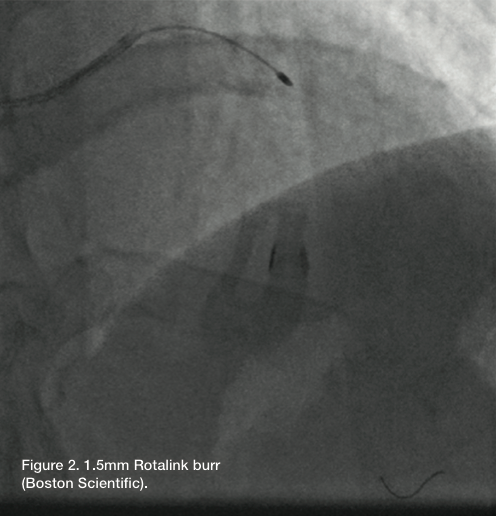
 A 1.5mm burr (RotaLink, Boston Scientific) was used to perform rotational atherectomy of the LAD. Total run time was about 30 seconds. Following rotational atherectomy, the over-the-wire balloon was advanced distally and the RotaWire exchanged for a Wiggle wire (Abbott Vascular). We advanced the Runthrough wire as a buddy wire (removed prior to rotational atherectomy).
A 1.5mm burr (RotaLink, Boston Scientific) was used to perform rotational atherectomy of the LAD. Total run time was about 30 seconds. Following rotational atherectomy, the over-the-wire balloon was advanced distally and the RotaWire exchanged for a Wiggle wire (Abbott Vascular). We advanced the Runthrough wire as a buddy wire (removed prior to rotational atherectomy).
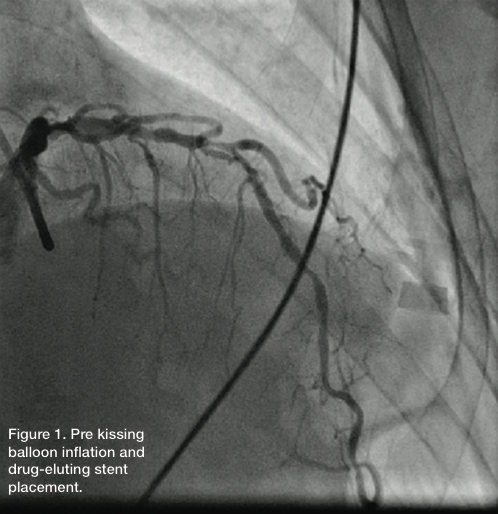
At this point, we were able to easily advance the 2.5 x  15mm AngioSculpt balloon. The LAD was predilated, with no significant compromise of the diagonal at this point. Following predilatation, a 2.75 x 20 Promus drug-eluting stent (Boston Scientific) was advanced and the buddy wire removed. The stent was deployed at 12 atm, followed by another inflation at 12 atm. The LAD had good flow, with an excellent angiographic result. However, there was compromise of the diagonal, which had no significant angiographic stenosis in the beginning, but 99% ostial disease.
15mm AngioSculpt balloon. The LAD was predilated, with no significant compromise of the diagonal at this point. Following predilatation, a 2.75 x 20 Promus drug-eluting stent (Boston Scientific) was advanced and the buddy wire removed. The stent was deployed at 12 atm, followed by another inflation at 12 atm. The LAD had good flow, with an excellent angiographic result. However, there was compromise of the diagonal, which had no significant angiographic stenosis in the beginning, but 99% ostial disease.
A Runthrough wire was advanced into the diagonal and a second Runthrough wire advanced distally into LAD. The Wiggle wire was removed. Kissing balloon angioplasty of the LAD and diagonal was performed. A 2.5 x 12 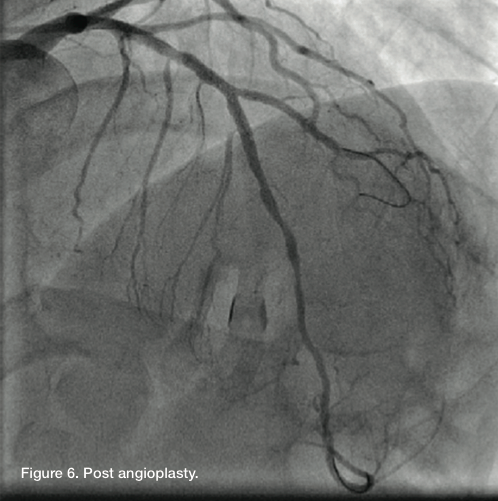 mm Apex balloon (Boston Scientific) was advanced into the diagonal and another 2.5 x 12 mm Apex balloon into the LAD. We inflated the diagonal at 6 atm, came down and then did kissing balloon inflation at 8 atm in both vessels. There was an excellent angiographic result, with TIMI-3 flow in both vessels and a residual of less than 20% in the ostial diagonal.
mm Apex balloon (Boston Scientific) was advanced into the diagonal and another 2.5 x 12 mm Apex balloon into the LAD. We inflated the diagonal at 6 atm, came down and then did kissing balloon inflation at 8 atm in both vessels. There was an excellent angiographic result, with TIMI-3 flow in both vessels and a residual of less than 20% in the ostial diagonal.  Orlando Marrero can be contacted at orlm8597@yahoo.com.
Orlando Marrero can be contacted at orlm8597@yahoo.com.
Dr. Zaheed Tai can be contacted at zaheedtai@gmail.com.
