


Transradial Intervention of a Saphenous Vein Graft
Case report
An 82-year-old male with a history of three-vessel coronary artery bypass surgery (CABG) 18 years prior underwent cardiac catheterization for the evaluation of non-ST elevation myocardial infraction (MI). Angiography revealed severe native coronary artery disease and two of the three vein grafts were occluded. His only patent conduit was a saphenous vein graph (SVG) to the left anterior descending (LAD) artery, which had a thrombotic sub-total occlusion. He was treated with a drug-eluting stent to the proximal segment of his vein graft. The patient did well and was subsequently discharged.
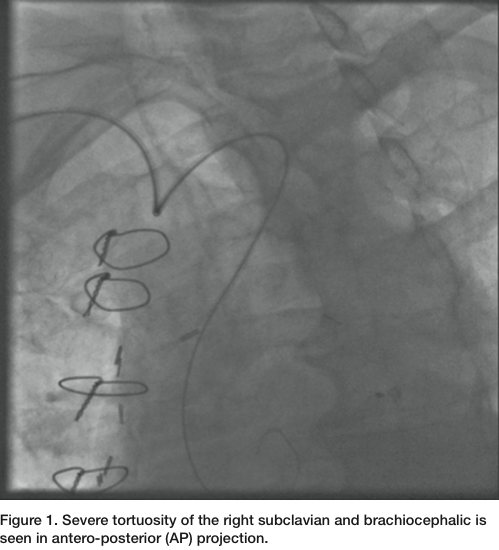 Three months later, the patient presented again with unstable angina. He has been compliant with his clopidogrel and aspirin. He had dynamic ST-T changes, without any elevation of cardiac enzymes. He was brought back to the cardiac catheterization laboratory. Diagnostic images were obtained with Judkins left (JL) 3.5 and Judkins right (JR) 4.0 diagnostic catheters through a 6 French (Fr) Glide sheath (Terumo) access in the right radial artery (RA). The patient had a very tortuous right subclavian and brachiocephalic arteries (Figure 1). The native LAD had a proximal chronic total occlusion. The SVG to LAD demonstrated a patent proximal stent, but with a
Three months later, the patient presented again with unstable angina. He has been compliant with his clopidogrel and aspirin. He had dynamic ST-T changes, without any elevation of cardiac enzymes. He was brought back to the cardiac catheterization laboratory. Diagnostic images were obtained with Judkins left (JL) 3.5 and Judkins right (JR) 4.0 diagnostic catheters through a 6 French (Fr) Glide sheath (Terumo) access in the right radial artery (RA). The patient had a very tortuous right subclavian and brachiocephalic arteries (Figure 1). The native LAD had a proximal chronic total occlusion. The SVG to LAD demonstrated a patent proximal stent, but with a 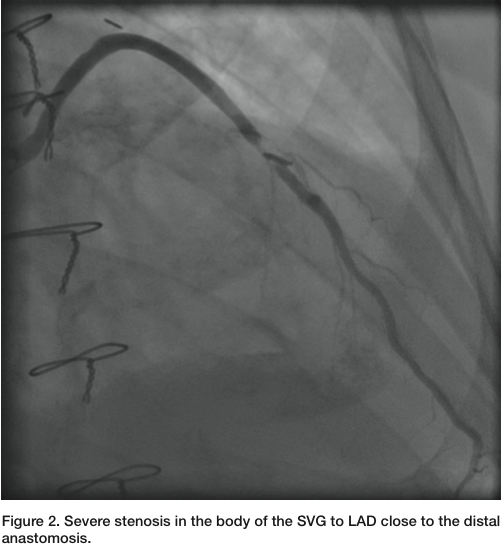 90% eccentric focal stenosis in the distal portion of the vein graft, very close to the anastomosis (Figure 2). Weight-based bivalirudin was initiated and a 6 Fr AL1 guide was used to cannulate the SVG to LAD. Though the severe tortuosity caused the cannulation of the graft to be challenging, a very co-axial supportive guide position was achieved (Figure 3, Figure 5). The lesion was crossed with a Kinetix wire (Boston Scientific). Due to the proximity of the lesion to the anastomosis, no distal protection device was deployed. A 3.5mm x 12mm Resolute drug eluting
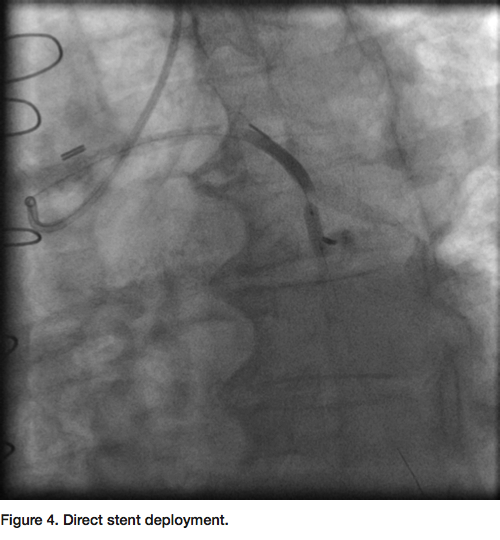
90% eccentric focal stenosis in the distal portion of the vein graft, very close to the anastomosis (Figure 2). Weight-based bivalirudin was initiated and a 6 Fr AL1 guide was used to cannulate the SVG to LAD. Though the severe tortuosity caused the cannulation of the graft to be challenging, a very co-axial supportive guide position was achieved (Figure 3, Figure 5). The lesion was crossed with a Kinetix wire (Boston Scientific). Due to the proximity of the lesion to the anastomosis, no distal protection device was deployed. A 3.5mm x 12mm Resolute drug eluting 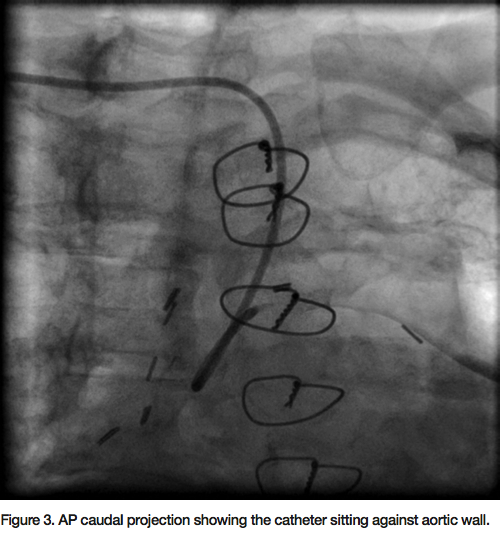 stent (DES) (Medtronic) was deployed at high pressure directly to the lesion without pre-dilation (Figure 4). Repeat angiogram confirmed successful deployment of the stent with a TIMI-3 flow and no residual stenosis (Figure 5). The guide and sheath were removed and a hemostatic wrist compression device was applied for 2 hours. The patient tolerated the procedure well. There was no post-procedure increase in the cardiac enzymes and he was discharged home the next day.
stent (DES) (Medtronic) was deployed at high pressure directly to the lesion without pre-dilation (Figure 4). Repeat angiogram confirmed successful deployment of the stent with a TIMI-3 flow and no residual stenosis (Figure 5). The guide and sheath were removed and a hemostatic wrist compression device was applied for 2 hours. The patient tolerated the procedure well. There was no post-procedure increase in the cardiac enzymes and he was discharged home the next day.
Discussion
 The advantages of complete revascularization with coronary artery bypass surgery are offset by limited long-term success with augmented atherosclerosis of the saphenous vein graft (SVG) after its use as a bypass conduit. PREVENT IV investigators reported 41.7% occlusion of one or more SVG grafts at the end of one year.1 Repeat surgical revascularization is associated with higher morbidity and mortality, and is challenged by the difficulty in finding surgical conduits in many patients. Therefore, percutaneous intervention (PCI) of the SVG is the favored
The advantages of complete revascularization with coronary artery bypass surgery are offset by limited long-term success with augmented atherosclerosis of the saphenous vein graft (SVG) after its use as a bypass conduit. PREVENT IV investigators reported 41.7% occlusion of one or more SVG grafts at the end of one year.1 Repeat surgical revascularization is associated with higher morbidity and mortality, and is challenged by the difficulty in finding surgical conduits in many patients. Therefore, percutaneous intervention (PCI) of the SVG is the favored 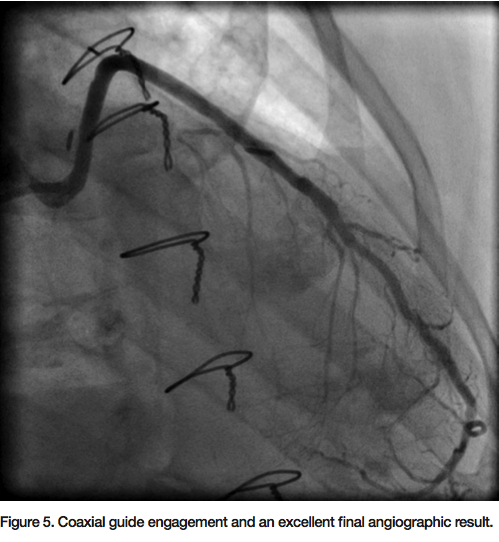 revascularization choice. The SVG intervention is technically challenging and is associated with higher rates of periprocedural MI, in-hospital mortality, restenosis, and occlusion compared with PCI of native coronary arteries.2 Degenerated friable lesions in a SVG lead to distal embolization of debris with no-flow or slow-flow phenomena, and are associated with increased post-PCI MI and mortality.3 Embolic protection device use is recommended as a Class I indication during SVG interventions. Similar to the case reported herein, the lack of a safe landing zone within the SVG prohibits the use of the distal protection device.
revascularization choice. The SVG intervention is technically challenging and is associated with higher rates of periprocedural MI, in-hospital mortality, restenosis, and occlusion compared with PCI of native coronary arteries.2 Degenerated friable lesions in a SVG lead to distal embolization of debris with no-flow or slow-flow phenomena, and are associated with increased post-PCI MI and mortality.3 Embolic protection device use is recommended as a Class I indication during SVG interventions. Similar to the case reported herein, the lack of a safe landing zone within the SVG prohibits the use of the distal protection device.
The most frequent reason for adverse clinical events after initial SVG intervention is disease progression at untreated, intermediate lesions.4 The lesion treatment we report herein was seen as an intermediate lesion on the angiogram three months prior to this procedure. Guided by multiple studies, including ISAR-CABG5, we preferentially use drug-eluting stents for the treatment of SVG, unless there are patient-specific limitations.
In the past, vein graft interventions via the radial approach were considered a relative contraindication. More recently, the transradial approach for SVG PCI has been seen to be feasible, safe, and as quick as the femoral approach. With the radial approach, the procedural success is high with similar radiation and contrast exposure, and it significantly lowers vascular complications in high-volume radial centers.6 SVG intervention remains one of the technically challenging subsets of transradial procedures. The following tips may help readers expand their radial use for SVG interventions.
1) A diagnostic angiogram for post-CABG patients is preferred via left radial access over the right, for the ease of left internal mammary artery (LIMA) cannulation. If the left radial artery was utilized as a bypass conduit, the right radial artery can be used. (Techniques to cannulate the LIMA from the right radial artery will be discussed in the future case report.) A JR 4 catheter can be used for a SVG angiogram from the left radial. The Tiger catheter (Terumo) works well as a universal catheter from the left radial access. From the right radial, the Jacky catheter (Terumo) works better, because of the tip with a modified Amplatz curve.
2) For SVG PCI, many radialists prefer the left radial artery approach over the right, as the graft anastomoses in the aorta are close to the origin of the brachiocephalic artery, which makes it difficult to engage with a guide. Although right radial artery access is challenging, once successfully engaged, an Amplatz Left (AL) 1 or AL2 catheter will seat against the arch of the aorta and provide firm support.
3) From either radial access site, AL guides are a better choice for PCI of SVG to the left coronary circulation. AL2 works better from the left radial artery and AL1 is more likely to work from the right radial artery. Unlike the right radial, the left radial approach may not provide as much support. A GuideLiner catheter (Vascular Solutions) could be used to enhance support in complex, tortuous anatomy.
4) From the left radial artery, a SVG to the right coronary system is better treated with a multipurpose guide. It provides co-axial engagement and support. From the right radial artery, specifically in the presence of brachiocephalic tortuosity, an AL2 is the preferred guide.
5) A JL guide can be used from the left radial access in selected patients for treating a SVG to the left coronary system, with very solid support.
6) All of the distal protection devices can be used through a standard 6 French guide.
7) Left radial access is achieved from the left side of the patient. After access is obtained, the arm is adducted, the forearm is flexed, and the left wrist of the patient is brought close to or on top of the left groin. Soft support with a pillow is provided under the left arm. The procedure is then performed from the right side of the patient (similar to using a left groin access).
References
- Alexander JH, Hafley G, Harrington RA, et al; PREVENT IV Investigators. Efficacy and safety of edifoligide, an E2F transcription factor decoy, for prevention of vein graft failure following coronary artery bypass graft surgery: PREVENT IV: a randomized controlled trial. JAMA 2005; 294: 2446-2454.
- Lee MS, Park SJ, Kandzari DE, Kirtane AJ, Fearon WF, Brilakis ES, Vermeersch P, Kim YH, Waksman R, Mehilli J, Mauri L, Stone GW. Saphenous vein graft intervention. JACC Cardiovasc Interv 2011 Aug; 4(8): 831-843.
- Abbo KM, Dooris M, Glazier S, O’Neill WW, Byrd D, Grines CL, Safian RD. Features and outcome of no-reflow after percutaneous coronary intervention. Am J Cardiol 1995 Apr 15; 75(12): 778-782.
- Ellis SG, Brener SJ, DeLuca S, Tuzcu EM, Raymond RE, Whitlow PL, Topol EJ. Late myocardial ischemic events after saphenous vein graft intervention — importance of initially “nonsignificant” vein graft lesions. Am J Cardiol 1997 Jun 1; 79(11): 1460-4.
- Mehilli J, Pache J, Abdel-Wahab M, Schulz S, Byrne RA, Tiroch K, Hausleiter J, Seyfarth M, Ott I, Ibrahim T, Fusaro M, Laugwitz KL, Massberg S, Neumann FJ, Richardt G, Schömig A, Kastrati A; Is Drug-Eluting-Stenting Associated with Improved Results in Coronary Artery Bypass Grafts? (ISAR-CABG) Investigators. Drug-eluting versus bare-metal stents in saphenous vein graft lesions (ISAR-CABG): a randomised controlled superiority trial. Lancet 2011 Sep 17; 378(9796): 1071-1078.
- Rathore S, Roberts E, Hakeem AR, Pauriah M, Beaumont A, Morris JL. The feasibility of percutaneous transradial coronary intervention for saphenous vein graft lesions and comparison with transfemoral route. J Interv Cardiol 2009 Aug; 22(4): 336-340.
_______________________________________________
The authors can be contacted via Dr. Kintur Sanghvi at SanghviK@Deborah.org.
This article received a double-blind peer review from members of the Cath Lab Digest editorial board.
