


Transcatheter Aortic Valve Replacement at the Emory Structural Heart Disease and Valve Center
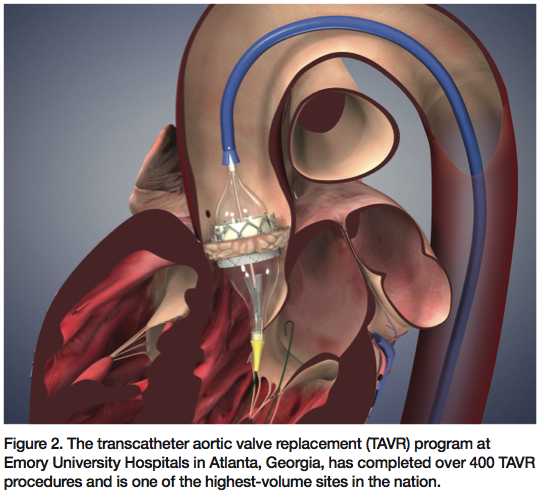
The transcatheter aortic valve replacement (TAVR) program at Emory University Hospitals in Atlanta, Georgia, has completed over 400 TAVR procedures and is one of the highest-volume sites in the nation.
Can you tell us about the Heart Team partnership at the Emory Structural Heart Disease and Valve Center?
 My introduction to transcatheter aortic valve replacement (TAVR) was via Peter Block, MD, FACC, who had done many of the early balloon aortic and mitral valvuloplasties in the United States. As a fellow under Dr. Block, I was encouraged to pursue further training in structural heart disease and he helped me contact Alain Cribier, MD, so I could spend 2004 to 2005 training in France. This was a very exciting time, as only a few cases of TAVR had been performed by Dr. Cribier and his team, and I was his first American fellow.
My introduction to transcatheter aortic valve replacement (TAVR) was via Peter Block, MD, FACC, who had done many of the early balloon aortic and mitral valvuloplasties in the United States. As a fellow under Dr. Block, I was encouraged to pursue further training in structural heart disease and he helped me contact Alain Cribier, MD, so I could spend 2004 to 2005 training in France. This was a very exciting time, as only a few cases of TAVR had been performed by Dr. Cribier and his team, and I was his first American fellow.
My passion for TAVR came from him. The TAVR project for me became very personal because it involved relationships between people — not only between me and the patients and their families, but also with my former mentors, Drs. Cribier and Block, trying to carry on their level of quality and service.
Upon my return to the United States, Dr. Block and I began working together as colleagues, building a large referral of structural heart disease patients to Emory, and re-started balloon aortic valvuloplasty in 2006. Around that time, I got a phone call from a young surgeon at Emory, Vinod Thourani, MD, who was talking about how important this technology was to him, how he loved valves and valve surgery, that he was going to China for a month to learn some catheter skills and asking whether we could make a team together. We formed a team made up of Robert Guyton, MD, the chief of surgery, Dr. Thourani, Dr. Block, and myself. Our first transfemoral implant was September 2007. In a year, we completed 30 implants and took a team trip to Leipzig, Germany, to watch Thomas Walther, MD, PhD, implant transapical valves.
Today, we have performed almost 400 TAVRs; Dr. Thourani and I have performed the majority of the implants. The team is incredibly efficient, with prompt implants, work-ups and turnarounds. We have added a considerable number of people to the team and have more help than in the early years, but Dr. Thourani and I still connect on every decision made, whether it is about the Emory Structural Heart Disease and Valve Center, or for a specifically tailored case with a complicated patient (which comes up quite frequently these days).
Our structure really works and is practical. One of the keys is that both cardiologists and surgeons are very passionate about TAVR and structural heart disease. We have learned from each other, and have been better as a whole than as individual parts. Our partnership has been unique because we are colleagues and friends, and have looked out for each other throughout the building process. It has also been important that our skill sets are complementary. In addition, it would have been hard to build a partnership without letting go of artificial boundaries and old traditions between surgeons and cardiologists.
Tell us about your TAVR clinic team. What dedicated resources do you have in place?
Our core TAVR clinic consists of two cardiologists (Dr. Block and me), two cardiac surgeons (Drs. Thourani and Guyton), and two TAVR coordinators (Patricia Keegan, NP, and Amy Simone, PA). We recently added two more cardiologists (Kreton Mavromatis, MD, and Chandan Devireddy, MD) and one more cardiac surgeon (Brad Leshnower, MD). Since 2007, we have had a cardiac fellow as part of the service (Mihir Kanitkar, MD), but we added cardiac surgical fellows last year (Tom Nguyen, MD, and Christian Shults, MD).
Perhaps one of the most important members of the team has been our echocardiographer, Stam Lerakis, MD, FAHA, FACC, FASE, FASNC, FCCP, who has really contributed a lot to interventional/procedural echo in the last few years. He has unlocked a lot of secrets for us in terms of sizing, paravalvular leak, transcatheter valve placement and problem solving. He reads the majority of our baseline and follow-up echos and did all the TAVR echos until last year, when we started performing TAVR at a second campus. He is also doing our cardiac CT, cardiac MRI and nuclear studies.
Also, until last year, we have had a dedicated sonographer (Sharon Howell, RDCS) and dedicated TAVR cath lab team (Kelly Broxton, RT(R)(CI), RCIS, and Jimmy Colgate, CVT EMT-P). We have one administrative assistant for the structural and valve center on each campus. The team is quite big now, with a very developed infrastructure.
In 2007, the TAVR clinic began with every patient seen the same day by the surgeon, cardiologist, and fellow, on one campus. This was very important, as we were learning from each other, and trying to set expectations for patients and patients’ families that would be agreeable to all parties involved in procedural planning. Since then, we have expanded to two campuses with TAVR coordinators, fellows, sonographers and echocardiographers, and hold clinic 3 to 4 days per week (new patients 2 days a week).
Currently, I run the TAVR clinic on one campus, while Dr. Thourani runs the TAVR clinic on the other campus. Once a week, previous patients and upcoming implants are reviewed by the heart team, and trouble-shooting and planning are done well before patients are scheduled for their procedures.
The sonographers have acquired so much experience — for example, a case of low-gradient aortic stenosis will prompt them to perform a dobutamine echo and patients with a large annulus measurement will often be studied by transesophageal echo (TEE). Our electronic archiving system creates a worksheet on every patient, with comments by the team; study results (CT, lower-extremity angiography, catheterization, echocardiography, carotid ultrasound, and pulmonary function tests) are captured on PowerPoint slides with representative pictures. The slides and worksheets are placed in folders, and the system lets us track 300 pre-implant patients easily. Patients seen in clinic who are candidates for further TAVR screening are scheduled for observation visits in the hospital if they are from far away or for outpatient tests if they are local. Patients are transferred frequently from other hospitals. We keep the lines of communication open with our referring doctors, and our cell phones are on 24/7 for urgent/emergent transfers and procedures.
How has your team educated your referring community about TAVR as an option for severe, symptomatic native aortic stenosis patients who meet the criteria for either the commercial indication or the PARTNER II Trial?
We started educating the community about TAVR in 2006 and have continued with several outreach projects, in-house lectures, and regional grand rounds every year. We have done national programs, proctoring, and fundamental courses to train new TAVR physicians. We educate cardiologists, internists, and cardiac surgeons on several levels.
We have increased our Internet footprint the last few years and do have a dedicated hotline number on the website. Our hospital operator routes physicians and patients to our offices when they receive calls regarding the TAVR program at Emory.
Emory is one of the highest-volume TAVR programs in the country. How has your TAVR program evolved over time?
 Early on, we recognized a need for timely evaluation and treatment of these very sick patients, so we added a second campus with access to a hybrid room 2 to 3 days per week. We hold TAVR clinic several times per week on both campuses, with two complete teams running at all times. With two fully trained teams, we have been able to do simultaneous implants in the hybrid OR and the cath lab. We have also done TAVR simultaneously on different campuses to deal with increasing volumes. Because these patients are suffering from severe aortic stenosis, it is important to be able to screen, triage, implant and discharge efficiently.
Early on, we recognized a need for timely evaluation and treatment of these very sick patients, so we added a second campus with access to a hybrid room 2 to 3 days per week. We hold TAVR clinic several times per week on both campuses, with two complete teams running at all times. With two fully trained teams, we have been able to do simultaneous implants in the hybrid OR and the cath lab. We have also done TAVR simultaneously on different campuses to deal with increasing volumes. Because these patients are suffering from severe aortic stenosis, it is important to be able to screen, triage, implant and discharge efficiently.
Walk us though the patient experience at Emory from the time of referral to the valve clinic, through the procedure, and on to discharge.
Referrals occur through our valve hotline, my office/cell phone or Dr. Thourani’s office/cell phone, or hospital admission/transfer. Patients are seen in the valve clinic. All outside records are reviewed, and a screening worksheet is made in advance. Any potential data discrepancies or exclusion criteria are identified, and tests are often ordered the same day as the office visit to verify or re-evaluate data from outside hospitals. Most often, the transthoracic echo is repeated the day of the office visit to give us more detailed anatomical and functional information.
If patients are reasonable candidates for TAVR, they are admitted for observational stays in the hospital. They undergo a series of tests (heart catheterization with lower extremity angiography, pulmonary function tests, carotid ultrasound, and CT scan). During their hospital stays, patients are seen by both the cardiologist and cardiac surgeon and are evaluated by both specialties.
If patients are too sick to be sent home, they are kept for TAVR or undergo balloon aortic valvuloplasty to bridge them to a more definitive therapy. Surgical patients who are not TAVR candidates may be operated upon during that hospital stay. In short, we try to have a definitive plan or give the patients a date for future TAVR or surgery before they go home.
All discharged patients are educated on aortic stenosis. They know to come back to Emory before their symptoms significantly worsen and are given detailed contact information before leaving. Our TAVR nurse coordinators are often the first points of contact for patients and families after the initial visit.
Patients are re-admitted the day before their procedures, and we meet with each patient and family the night before the procedure to answer any final questions or address any new issues. We are very aware that communication with spouses and every member of the immediate family is critically important.
After the procedure, we immediately communicate with the referring physician and the patient’s family. We admit them to the ICU the first night and often transfer to a regular floor bed the next day. We often initiate a social service consult the first post-operative day to evaluate patients for short-term rehab, home physical therapy, home health assistance, and the like. Upon discharge, a 1-month follow-up appointment is scheduled. Study patients are seen by study coordinators for discharge testing.
How has post-procedure care evolved over time?
We currently have an ICU team that takes care of patients immediately post-TAVR. This team is run either by a cardiac anesthesiologist or a cardiologist. This team also consists of mid-level providers, fellows, and residents, and we have provided TAVR education monthly to keep the teams informed about expected outcomes, procedural approaches, and changes in protocols or devices. The TAVR team remains involved with patients during their ICU stay, then resumes care when they are transferred back to the floor.
We have learned to anticipate many of the common problems of performing hybrid procedures on the elderly: nutrition, delirium, fall risks and mobility limitations, anticoagulation risks and social needs (long-term and short-term rehabilitation). The post-op care (and the anticipation of problems before they occur) is critically important, as is patient selection and careful procedural techniques.
We have also gotten more aggressive with the evaluation and treatment of paravalvular leak (PVL). If patients are not progressing within the hospital stay or by one-month post-TAVR, we carefully re-assess the degree of PVL, which is often difficult, by transthoracic echo (TTE).
How has your approach to the TAVR procedure evolved over time?
Dr. Cribier has spent a lifetime understanding aortic stenosis, and taking a complex therapy and making it simple. We have adopted the same philosophy at Emory and continue to collaborate with Dr. Cribier and his team to this day.
I think one of the key collaborations between the two groups has been the use of balloon sizing of the aortic annulus to select transcatheter valve size. We have published two papers on this topic1,2, identifying the balloon used during the valvuloplasty as a valve sizer, exactly as a surgeon would use for traditional surgical AVR. We adopted a completely percutaneous approach by 2009 with the 22 French (Fr) and 24 Fr devices, and have minimized vascular screening to a non-contrast CT and lower-extremity angiogram (10 cc of contrast). In patients with renal insufficiency, we have decreased the total contrast use to 20 cc per procedure by using the echo and the pigtail catheter placed on the aortic valve to determine the valve plane and position. We have started transporting patients to a telemetry floor and have avoided ICU stays completely in some cases.
What advice would you give to centers that are gearing up to begin a TAVR program?
The toughest period for a new TAVR center is the first 10 implants. The first 10 procedures should be successful, to gain the confidence of referring physicians and hospital staff. It is often tough to find 10 “perfect” patients for TAVR, especially early in one’s experience, and the temptation to try an implant in a non-ideal situation is very strong. It is important for new centers to resist this urge and send some of these patients for smaller devices and transapical approach in experienced centers that are part of clinical trials. Also, it is important for new centers to evaluate and treat the patient with severe, symptomatic aortic stenosis efficiently, as delays can result in mortality.
Over time, a new center should expect the number of cases to grow. Organization is a critical part of these programs, and a smart TAVR nurse coordinator can help immensely in this area. Also, the team is only as strong as its weakest link. A hybrid program such as TAVR cannot be built on the back of only one cardiologist or one cardiac surgeon or one echocardiographer, regardless of skill level. The trick is to find all three, in one center, who are very capable and like working together.
References
- Babaliaros VC, Liff D, Chen EP, et al. Can balloon aortic valvuloplasty help determine appropriate transcatheter aortic valve size? JACC Cardiovasc Interv 2008 Oct; 1(5): 580-586.
- Babaliaros V, Junagadhwalla Z, Lerakis S, et al. Use of balloon aortic valvuloplasty to size the aortic annulus prior to implantation of a balloon-expandable transcatheter heart valve. JACC Cardiovasc Interv 2010 Jan; 3(1):114-118.
- Lerakis S, Babaliaros VC, Block PC, et al. Transesophageal echocardiography to help position and deploy a transcatheter heart valve. JACC Cardiovasc Imaging 2010;3(2):219-221.
