


TAVR – A Personal Experience
The patient
I have a very close family acquaintance with aortic stenosis who was beginning to fail. I have known this 91-year-old widowed woman and mother of 4 for many years. Mrs. KJ had a past history of hypertension, atrial fibrillation requiring atrioventricular (AV) nodal ablation and a pacemaker. She had diet-controlled diabetes and arthritis. She had been experiencing progressive dyspnea on exertion over 5 years and was diagnosed with left ventricular hypertrophy (LVH) and diastolic dysfunction and mild calcific aortic stenosis until recently. An aortic valve replacement was recommended several years ago, but she refused to consider this option. She believed the surgery was “too much” for her. Medical therapy for hypertension did not relieve symptoms.
known this 91-year-old widowed woman and mother of 4 for many years. Mrs. KJ had a past history of hypertension, atrial fibrillation requiring atrioventricular (AV) nodal ablation and a pacemaker. She had diet-controlled diabetes and arthritis. She had been experiencing progressive dyspnea on exertion over 5 years and was diagnosed with left ventricular hypertrophy (LVH) and diastolic dysfunction and mild calcific aortic stenosis until recently. An aortic valve replacement was recommended several years ago, but she refused to consider this option. She believed the surgery was “too much” for her. Medical therapy for hypertension did not relieve symptoms.
Her long-standing cardiologist retired and her new younger cardiologist reviewed her history and current symptoms, and repeated an echocardiogram, finding severe aortic stenosis with valve area of <0.6cm2, pulmonary hypertension (estimated around 60mmHg), very large left atrium, but normal LV function with concentric LVH. Upon further discussion, he recommended a transcatheter aortic valve replacement (TAVR), because of recent clinical deterioration alongside dyspnea at rest with an inability to walk more than 10 steps. No chest pain or syncope was noted. She and her family asked me about the TAVR procedure. After speaking to the referring and potential treating cardiologists, I talked to her and her children and grandchildren, and explained what I knew about benefits (marked relief of symptoms and reduced complications from open heart surgery) and risks (stroke, bleeding, and death), and that I thought this was a good idea if performed by an experienced operator and team. She agreed to proceed, as long as she could get the procedure in time to attend her granddaughter’s wedding several months later. She and the family asked me to help get this done. I said, “I’ll see what I can do.”
normal LV function with concentric LVH. Upon further discussion, he recommended a transcatheter aortic valve replacement (TAVR), because of recent clinical deterioration alongside dyspnea at rest with an inability to walk more than 10 steps. No chest pain or syncope was noted. She and her family asked me about the TAVR procedure. After speaking to the referring and potential treating cardiologists, I talked to her and her children and grandchildren, and explained what I knew about benefits (marked relief of symptoms and reduced complications from open heart surgery) and risks (stroke, bleeding, and death), and that I thought this was a good idea if performed by an experienced operator and team. She agreed to proceed, as long as she could get the procedure in time to attend her granddaughter’s wedding several months later. She and the family asked me to help get this done. I said, “I’ll see what I can do.”
The evaluation
Because Mrs. KJ lives in southern California, I called my colleague Dr. Raj Makkar at Cedars- Sinai Medical Center, who agreed to see her, have her evaluated and if suitable, have her undergo TAVR. Dr. Makkar and his team have done more TAVR procedures than anyone in the country. He was gracious enough to get her an early appointment for evaluation and consultation to be considered as a TAVR candidate.
Sinai Medical Center, who agreed to see her, have her evaluated and if suitable, have her undergo TAVR. Dr. Makkar and his team have done more TAVR procedures than anyone in the country. He was gracious enough to get her an early appointment for evaluation and consultation to be considered as a TAVR candidate.
Mrs. KJ’s daughter took her to Cedars-Sinai Medical Center, where she was evaluated by Dr. Makkar and his team after obtaining a CT scan, 2D echo, ECG, and blood work. The following day she was seen by the cardiologists and, as the procedure is part of a ‘heart team’ approach, a cardiothoracic surgeon. [Interestingly, she reported that the surgeon told her she had high surgical risk (as was expected) and that he was the one that was going to implant the valve, confusing her about who was really doing the job.] Nonetheless, the CT scan showed she had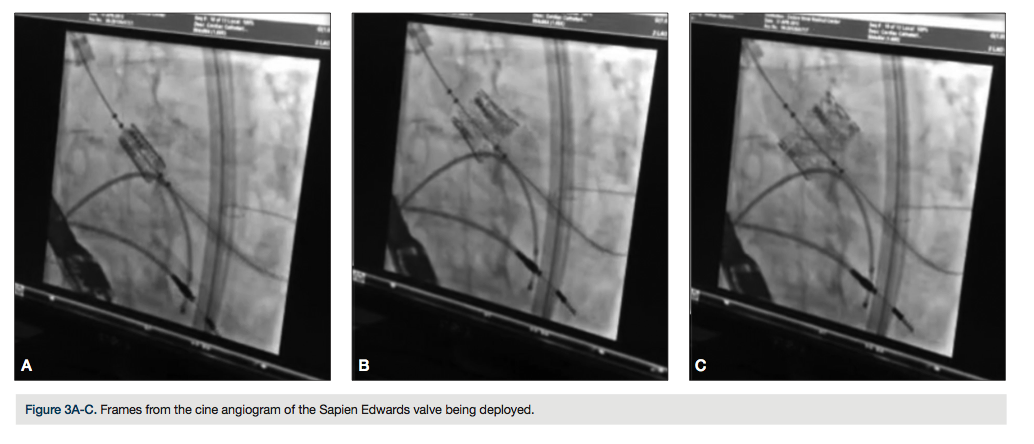 little calcification of any of her major arteries, including the iliac arteries and aortic arch and ascending aorta. Further analysis of the CT scan also showed she had an aortic root suitable of accepting a large Sapien Edwards 26mm valve. Echocardiography confirmed previous findings of pulmonary hypertension, very large left atrium, mild mitral regurgitation and normal left ventricular function. In other words, Mrs. KJ was a good TAVR candidate with high surgical risk, and she was ready to proceed the next day.
little calcification of any of her major arteries, including the iliac arteries and aortic arch and ascending aorta. Further analysis of the CT scan also showed she had an aortic root suitable of accepting a large Sapien Edwards 26mm valve. Echocardiography confirmed previous findings of pulmonary hypertension, very large left atrium, mild mitral regurgitation and normal left ventricular function. In other words, Mrs. KJ was a good TAVR candidate with high surgical risk, and she was ready to proceed the next day.
The hospital admission
Mrs. KJ signed in to the hospital and was processed through the usual admission paperwork. Because of my close association with the family and because I was also curious exactly what was it like to be a patient having a TAVR, I accompanied the family throughout the hospital stay.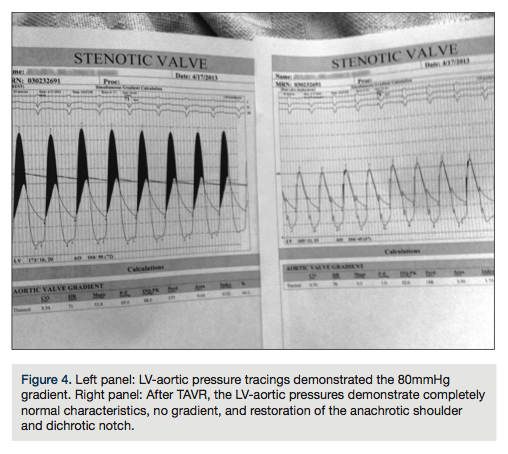 Mrs. KJ had a detailed advanced health care directive (something we should all have whenever we enter a hospital). At 8:00 am, she was taken into the holding area of the cath lab to be prepared for the procedure. It was interesting that in this day of modern electronic medical records, there were 8 separate paper consent forms with multiple copies which required her signature (Figure 1). After placing the intravenous lines, she was visited by the anesthesiologist, cardiology fellow, cardiology attending physician, and several nurses before being taken into the cath lab.
Mrs. KJ had a detailed advanced health care directive (something we should all have whenever we enter a hospital). At 8:00 am, she was taken into the holding area of the cath lab to be prepared for the procedure. It was interesting that in this day of modern electronic medical records, there were 8 separate paper consent forms with multiple copies which required her signature (Figure 1). After placing the intravenous lines, she was visited by the anesthesiologist, cardiology fellow, cardiology attending physician, and several nurses before being taken into the cath lab.
Into the cath lab
I stayed outside the lab with the family to lend support. Although I had full confidence in the operating team, as I was familiar with all aspects of the cath lab, from the family’s view, this was a terrifying procedure that might be the last time they see their mother, an understandably frightening event. I provided as much moral support as I could. Afterward, I gained an even greater appreciation on a personal basis for how much support the cath lab team members provide to families. This support is an immense comfort to the families of those patients having both routine and advanced cath procedures. At 11:30 am, the procedure was completed successfully. She was extubated in the cath lab and transferred to the ICU for monitoring.
The results of TAVR
While I was not in the cath lab during the procedure, the cardiology fellow, Dr. Manchury, kindly shared the hemodynamics and angiographic data from the procedure. I was awestruck by the results. Before sharing the results here, I want to review the steps of the procedure. I am sure there are different routines at different hospitals and for different types of patients regarding how TAVR is performed, but I will share what the routine was for this patient in this practice.
The first part of the procedure was establishing excellent bilateral femoral access using micro puncture technique, confirmed by angiography. Both access sites were in the common femoral arteries, which were not calcified or excessively tortuous. The next part was an abbreviated coronary angiographic and aortic root study (her creatinine was 1.4mg/dl). Following the angiography, a temporary transvenous pacemaker is positioned, even though she has a well-functioning DDD pace maker of her own. The pacer was to be used for the rapid ventricular pacing needed to reduce left ventricular ejection force, permitting more stable balloon inflation across the aortic valve. After crossing the aortic valve with a stiff guide wire, aortic balloon dilation was performed. The 4cm x 20mm balloon catheter was then exchanged for the Sapien Edwards stent 26mm valve system and during rapid ventricular pacing (180bpm), the stent valve is deployed (Figure 2), and the catheter is removed. Hemodynamics are measured before and after the implant. When Dr. Manchury showed me the hemodynamics, I was thrilled (Figure 3). Before TAVR, the left ventricular-ascending aortic (LV-Ao) gradient was nearly 80mmHg, and as is easily seen, after TAVR, the gradient is not only abolished, but there is restoration of a completely normal aortic pressure contour and matching LV tracing, including the anachrotic shoulder as well as a distinct dichrotic notch, neither feature present before implanting the valve.
pacing needed to reduce left ventricular ejection force, permitting more stable balloon inflation across the aortic valve. After crossing the aortic valve with a stiff guide wire, aortic balloon dilation was performed. The 4cm x 20mm balloon catheter was then exchanged for the Sapien Edwards stent 26mm valve system and during rapid ventricular pacing (180bpm), the stent valve is deployed (Figure 2), and the catheter is removed. Hemodynamics are measured before and after the implant. When Dr. Manchury showed me the hemodynamics, I was thrilled (Figure 3). Before TAVR, the left ventricular-ascending aortic (LV-Ao) gradient was nearly 80mmHg, and as is easily seen, after TAVR, the gradient is not only abolished, but there is restoration of a completely normal aortic pressure contour and matching LV tracing, including the anachrotic shoulder as well as a distinct dichrotic notch, neither feature present before implanting the valve.
Post procedure
In the afternoon, I joined the family to visit Mrs. KJ in her room. She felt much better and had no discomfort of any kind, including her femoral access sites (one Angio-Seal, one with double Perclose) and the internal jugular sheath. She said she could breathe better as we observed her during conversations and she was able to eat without being short of breath. Of interest, she had hypertension after the TAVR with a much higher blood pressure (190/100) than she had before the procedure, which required increasing anti-hypertensive drugs. That night at home, I found a paper demonstrating that those patients with a hypertensive response after TAVR compared to those who did not increase or had reduced blood pressure had better 3-year survival.1
The hospital discharge and follow-up
In the morning of the next day, Mrs. KJ could walk 50 steps before lunch, then 100 steps late in the day, without difficulty. She was discharged that evening (Figure 5). She has done remarkably well, with reports of continued increased activity, but to a limit. She still has exertional dyspnea, but at a much increased activity level. Recall that before aortic stenosis was diagnosed, she had dyspnea on exertion due to hypertension, diastolic dysfunction, and atrial fibrillation. Mrs. KJ will certainly enjoy a better quality of life for a time and that was the goal. She and her family also wanted to thank Dr. Makkar and his team for a job well done. This case exemplifies the very best of what I believe interventional cardiology and the cath lab is all about.
I asked Mrs. KJ if I could write her story and show her pictures. She said yes. All I could say was, “Thanks, Mom, for everything.”
Reference
- Perlman GY, Loncar S, Pollak A, et al. Post-procedural hypertension following transcatheter aortic valve implantation: Incidence and clinical significance. J Am Coll Cardiol Intv. 2013; Epub ahead of print.
