


Suggestions for Peripheral Intervention
 While our main purpose in the cardiac cath lab is diagnostic and interventional cardiology, we are seeing a great many peripheral cases being performed. The risk factors of coronary artery disease and peripheral arterial disease (PAD) overlap and it makes sense to screen and perform interventions on patients when indicated. Patients that have known coronary disease should also be evaluated for PAD.
While our main purpose in the cardiac cath lab is diagnostic and interventional cardiology, we are seeing a great many peripheral cases being performed. The risk factors of coronary artery disease and peripheral arterial disease (PAD) overlap and it makes sense to screen and perform interventions on patients when indicated. Patients that have known coronary disease should also be evaluated for PAD.
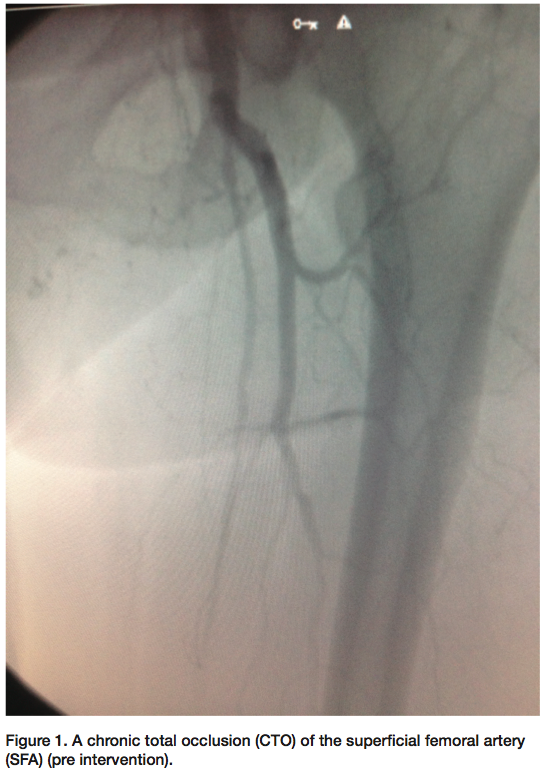
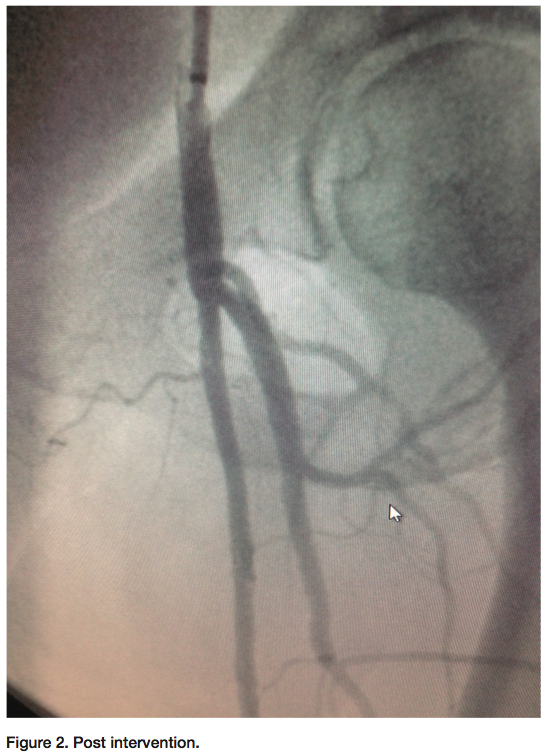 Some of the peripheral cases we perform include chronic total occlusions (CTOs) of the superficial femoral artery (SFA) (Figure 1-2). It may take some time crossing with a wire or crossing device on the proximal cap of the CTO. If trying to cross the CTO cannot be accomplished on the proximal cap of the SFA, gaining access distally may be a better option. Gaining access from a pedal or popliteal artery site is becoming more common. As we perform these interventions, we have access to the distal vessels to manipulate the guidewire up through the CTO from the distal cap first. Crossing the CTO with success from the distal cap works nicely most of the time. We have seen that the distal cap of the occlusion tends to be more crossable than the proximal cap. Once crossed and with verification that the wire is in the lumen of the vessel, the decision is made on what size sheath will be inserted. Depending on whether there are multiple lesions other than the CTO of the SFA, and whether your working access point is going to be from the distal access or from the femoral area, it might require a larger-size sheath. If you choose to work from the femoral area that is probably already accessed from the diagnostic films, then wiring through the lesion and into the sheath that is already across the bifurcation of the iliacs is a good method. Since your wire will be exchange length, grasping the wire tip is easily done. This way, you always have wire access during the entire procedure. The physician’s interventional plans determine the course of action that will be taken. If your interventional plans require you to use a smaller or larger wire (depending on what wire is used to make the initial crossing), the wire can always be exchanged out for a different size. Once the CTO is opened with a balloon, you can always change out the wire using a catheter such as the Seeker Crossing Support catheter (Bard PV) (or the physician’s preferred catheter). This is normally done if the physician decides to use an intravascular ultrasound (IVUS) catheter or any other device that requires the wire to be changed out (Volcano has both an .014 and .038 IVUS catheter).
Some of the peripheral cases we perform include chronic total occlusions (CTOs) of the superficial femoral artery (SFA) (Figure 1-2). It may take some time crossing with a wire or crossing device on the proximal cap of the CTO. If trying to cross the CTO cannot be accomplished on the proximal cap of the SFA, gaining access distally may be a better option. Gaining access from a pedal or popliteal artery site is becoming more common. As we perform these interventions, we have access to the distal vessels to manipulate the guidewire up through the CTO from the distal cap first. Crossing the CTO with success from the distal cap works nicely most of the time. We have seen that the distal cap of the occlusion tends to be more crossable than the proximal cap. Once crossed and with verification that the wire is in the lumen of the vessel, the decision is made on what size sheath will be inserted. Depending on whether there are multiple lesions other than the CTO of the SFA, and whether your working access point is going to be from the distal access or from the femoral area, it might require a larger-size sheath. If you choose to work from the femoral area that is probably already accessed from the diagnostic films, then wiring through the lesion and into the sheath that is already across the bifurcation of the iliacs is a good method. Since your wire will be exchange length, grasping the wire tip is easily done. This way, you always have wire access during the entire procedure. The physician’s interventional plans determine the course of action that will be taken. If your interventional plans require you to use a smaller or larger wire (depending on what wire is used to make the initial crossing), the wire can always be exchanged out for a different size. Once the CTO is opened with a balloon, you can always change out the wire using a catheter such as the Seeker Crossing Support catheter (Bard PV) (or the physician’s preferred catheter). This is normally done if the physician decides to use an intravascular ultrasound (IVUS) catheter or any other device that requires the wire to be changed out (Volcano has both an .014 and .038 IVUS catheter).
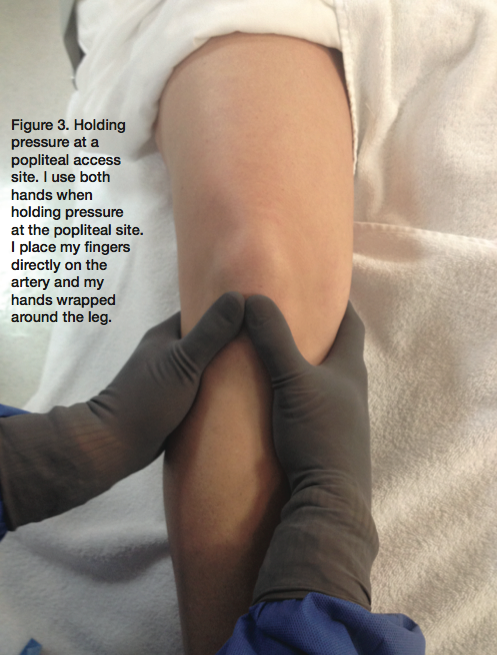 Once your intervention is finished, you will have two access points to close. If your femoral access point is suitable for a closure device, it is always a good way to close the artery. However, since these patients have peripheral disease, that area might not be suitable. If you used an access device such as Axera 2 (Arstasis, Inc.) in the beginning of the case, then waiting the appropriate time for the anticoagulation therapy before pulling the sheath is an acceptable choice. For your distal access point (such as pedal access), holding correct pressure is key. If the access was at the popliteal area, holding pressure must be with accurate precision. The technique for holding pressure at the popliteal site is up to the physician and the individual holding pressure. I use both hands when holding pressure at the popliteal site. I place my fingers directly on the artery and my hands wrapped around the leg (Figure 3). There are other acceptable ways of applying pressure as well. It depends on your facility and physician. Since holding at the popliteal site is different than holding pressure at other areas, you want to watch the area closely to ensure there is no bleeding behind the knee area. If bleeding occurs, there are a few options to stop it, including placing a covered stent at the access point to avoid surgery.
Once your intervention is finished, you will have two access points to close. If your femoral access point is suitable for a closure device, it is always a good way to close the artery. However, since these patients have peripheral disease, that area might not be suitable. If you used an access device such as Axera 2 (Arstasis, Inc.) in the beginning of the case, then waiting the appropriate time for the anticoagulation therapy before pulling the sheath is an acceptable choice. For your distal access point (such as pedal access), holding correct pressure is key. If the access was at the popliteal area, holding pressure must be with accurate precision. The technique for holding pressure at the popliteal site is up to the physician and the individual holding pressure. I use both hands when holding pressure at the popliteal site. I place my fingers directly on the artery and my hands wrapped around the leg (Figure 3). There are other acceptable ways of applying pressure as well. It depends on your facility and physician. Since holding at the popliteal site is different than holding pressure at other areas, you want to watch the area closely to ensure there is no bleeding behind the knee area. If bleeding occurs, there are a few options to stop it, including placing a covered stent at the access point to avoid surgery.
There are multiple access points that can be used for interventional access. If trying to cross an ostial iliac lesion, another access point is through the arm. Occasionally, if there is an ostial lesion of the iliac artery, using a crossover catheter (Cordis) might not supply enough support. If accessed from the arm, a long sheath can be placed closer to the lesion for more support.
These are a few techniques that are used in our lab. There are a number of ways to intervene on lesions and I have shared our experience with a few methods. If you are interested in more techniques or areas of interest for peripheral cases, I would be happy to assist.
If you have a subject you would like covered or an area of interest, please contact Phillip Mumford, RCIS, at p_mumford@aol.com.
Follow Phillip on Twitter: @phillip_mumford
