


Structuring a Transcatheter Aortic Valve Replacement Program
 Transcatheter aortic valve replacement (TAVR) is currently indicated to treat patients with severe symptomatic native aortic valve stenosis who are deemed ineligible for surgery. Medical City Dallas Hospital’s Dallas Valve Institute and Cardiopulmonary Research Science and Technology Institute (CRSTI) is one of the leading TAVR programs in the United States for treating these very sick patients, who historically have not been referred for consideration for aortic valve replacements.
Transcatheter aortic valve replacement (TAVR) is currently indicated to treat patients with severe symptomatic native aortic valve stenosis who are deemed ineligible for surgery. Medical City Dallas Hospital’s Dallas Valve Institute and Cardiopulmonary Research Science and Technology Institute (CRSTI) is one of the leading TAVR programs in the United States for treating these very sick patients, who historically have not been referred for consideration for aortic valve replacements.
Can you tell us about your TAVR program and its structure?
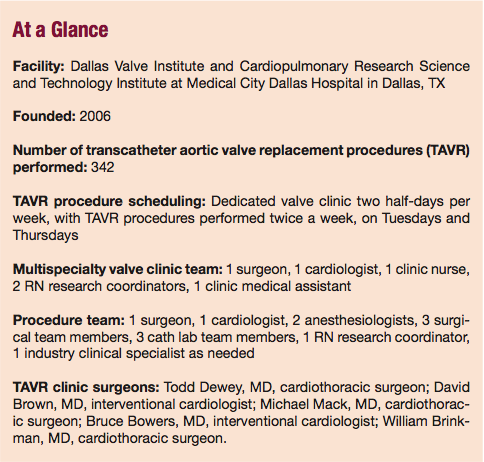
Angela G. Riley, RT: We started out in the interventional cardiologist’s office and evolved into a hospital-based outpatient clinic. We moved to the full valve clinic with a goal of easing the process for the patients, so they could have everything done in one facility over a short period of time. Currently, we’re seeing 10 to 12 new patients each week and 6 to 10 follow-up patients per week.
On our valve clinic days, all diagnostic testing is done in the morning. When the physicians are ready to see a patient in the afternoon, the computerized tomography angiography (CTA), the echocardiogram, and all other information is available. The physician will then review all the diagnostic tests.
Where do things go from there?
Jill Fowler, RN, BSN, CCRC: The physicians can give the patients a good idea of what treatment options they have at that time. This prevents multiple trips to our center; instead, over a Tuesday and Wednesday, the patient can have a complete answer regarding treatment options. We also send follow-up letters to referring physicians after clinic sessions with plans of care for their patients.
How do you identify patients who are good candidates for TAVR?
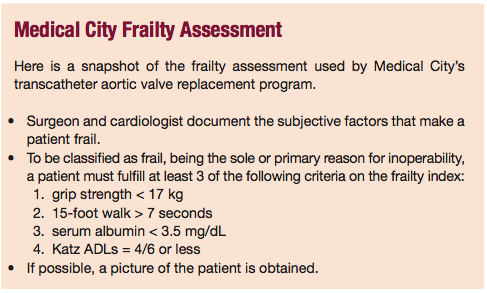
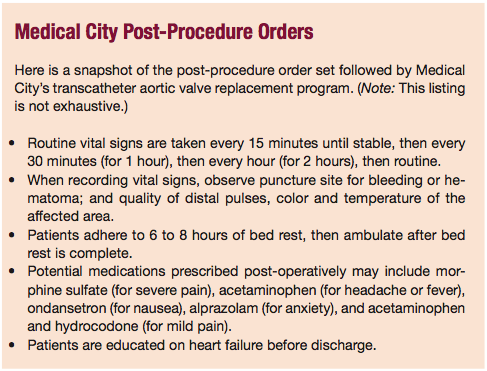
 Ms. Fowler: We use a frailty assessment (see Medical City Frailty Assessment), and look at CTA scans for arterial diameter measurements — iliac femoral for more than 7 mm. We perform an echocardiogram to confirm that the patient has critical aortic stenosis and check pulmonary function tests to monitor lung status. We use diagnostic order sets, an echo protocol, a CTA protocol, a renal protocol and a post-TAVR order (see Medical City Post-Procedure Orders) to identify, assess and manage TAVR patients. It’s really about looking at a full picture of the patient to see what treatment option, if any, can be pursued.
Ms. Fowler: We use a frailty assessment (see Medical City Frailty Assessment), and look at CTA scans for arterial diameter measurements — iliac femoral for more than 7 mm. We perform an echocardiogram to confirm that the patient has critical aortic stenosis and check pulmonary function tests to monitor lung status. We use diagnostic order sets, an echo protocol, a CTA protocol, a renal protocol and a post-TAVR order (see Medical City Post-Procedure Orders) to identify, assess and manage TAVR patients. It’s really about looking at a full picture of the patient to see what treatment option, if any, can be pursued.
Ms. Riley: Patients are split into four groups: too healthy, good candidate, marginal candidate or too-sick/poor candidate for TAVR. Too-healthy patients are offered conventional surgery, and our surgeons communicate with the referring physicians about this. Too-sick patients receive medical management. We might offer them a balloon valvuloplasty, but explain that it’s a temporary solution, and the aortic stenosis will reoccur in time.
Marginal candidates may be frail or may have low ejection fraction. The patients are scheduled in the cardiac cath lab for a potential balloon aortic valvuloplasty (BAV), to get them well enough for the TAVR procedure. So we’ll see them back in the clinic 30 days after the BAV to see if they can qualify for TAVR.
Good candidates are scheduled for the TAVR procedure. In the meantime, we’ll inject dye into the coronaries to see if they have any blockages, do an iliac runoff to assess whether the iliac vessels can accommodate the device, and perform other pre-operative preparations.
Tell us about your extended heart team. Who is on the team, what are their roles and responsibilities, and how do they interact during the course of patient treatment?
 Ms. Riley: The valve program nurse manager oversees all program functions and is the primary person who handles patient screening, gathers medical records, schedules pre-diagnostic testing and valve clinic appointments, and communicates with internal and external physicians.
Ms. Riley: The valve program nurse manager oversees all program functions and is the primary person who handles patient screening, gathers medical records, schedules pre-diagnostic testing and valve clinic appointments, and communicates with internal and external physicians.
Jennifer Ledbetter, RN, BSN: The valve clinic nurse provides support from our research arm by, for example, answering questions about medications such as bridging anticoagulants, and fielding calls for follow-up appointments either in the valve clinic or with the referring physicians.
We also recruited someone in a medical assistant (MA) role, and she does scheduling and registration as well, to help facilitate coordinating the scheduling of physician, OR and cath lab team time. She also makes sure all diagnostic tests are scheduled for the morning valve clinic visit and helps on the hospital side by ensuring all critical information is available for insurance precertification. Finally, the MA helps the valve clinic nurse do charting, vital signs and filing, so she is sort of a jack of all trades.
We’ve had nurse practitioners (NPs) all along, but we want to add an outpatient NP to help with expanding the valve clinic and perhaps in adding another procedure day. It will help us if we need patients to come in for visits that don’t necessarily require physician involvement.
Ms. Fowler: My background is research, and my role has evolved into the valve program manager. The doctors call me the “traffic cop” who manages the flow of the patients and the program. I receive calls from all new patients and referring physicians, review their medical records, schedule the appropriate testing, and see them in valve clinic.
Before we ever see the patients, I have a good idea what we’re going to be looking at. I put together a synopsis of each patient’s medical history for the physicians. I put everything in front of the physicians to help them decide which treatment options are best, then outline those treatment decisions to the patient. All the while, we communicate with the referring physician about the plan as well.
What is the composition of your program’s team of specialists?
Ms. Riley: We work with a pulmonologist, nephrologist, intensivist or gerontologist, and neurologist. They help manage patients’ co-morbid conditions.
Ms. Fowler: The average patient is very sick; 84 years old is the median age. So it’s important that you define your team of specialists at the program’s inception, because the extended team is critical for assisting the inpatient team in caring for these patients. Even if you grow into that model, as we did, it’s good to know where you’re going.
How have you been educating your referring community about TAVR as an option to treat these patients?
 Ms. Riley: We take our physicians out for local speaking opportunities. They do grand rounds at other hospitals and hold CME programs locally, and we purchase letter mailings (10,000) to send to cardiologists, cardiovascular surgeons and internal medicine specialists in Texas and the five surrounding states.
Ms. Riley: We take our physicians out for local speaking opportunities. They do grand rounds at other hospitals and hold CME programs locally, and we purchase letter mailings (10,000) to send to cardiologists, cardiovascular surgeons and internal medicine specialists in Texas and the five surrounding states.
Ms. Ledbetter: We also have the physicians speak at an annual community heart program in February. They talk to patients about minimally invasive TAVR, how the patients qualify, and highlight our healthy-eating restaurant program.
Ms. Fowler: Our TAVR program website is critical for highlighting what we’re doing. We work with the hospital marketing department to do patient stories and reach out to local media, geriatric magazines, and smaller community magazines and journals. One of our recent patients brought in an article she’d seen in Senior News — that’s how she found out about us.
What advice do you have for new TAVR coordinators?
Ms. Riley: Develop a tracking tool early to track patients and their referring physicians, such as an Excel spreadsheet or electronic medical records. This should track patient demographics (e.g., date of birth, social security number, telephone number), the source of the referral (e.g., Internet, media, physician lecture), the referring physician’s contact information, and the patient’s disposition. This lets us track the outcomes of our patients, along with where our referrals come from and which marketing techniques were successful.
Ms. Fowler: Each member of the team should have a clear, defined role, or else you’ll be either tripping over each other or not getting things done. We meet weekly to discuss issues with the program, and to see where everyone is and what everyone is focusing on.
Running a program like this requires diplomacy, because you’re working as the intermediary between cardiologists, cardiovascular surgeons, referring physicians, cath lab staff, OR staff, patients and families. It’s important to know the specialists you’ll be working and speaking with. In-service your hospital staff (such as telemetry units, occupational therapists and physical therapists) on the TAVR procedure and post-operative care of this patient population.
Ms. Riley: We compare it to a hospital’s setting up a heart-transplant program. Once patients are high-risk valve patients, they always are. We’re going to send them back to their referring cardiologists for other follow-up visits, but they will have annual visits with the valve clinic, similar to transplant programs.
What would you say your primary keys to success have been?
 Ms. Riley: I’d say the keys are a collegial working relationship between cardiologists and surgeons, and the other specialists involved; having a TAVR coordinator and inpatient NP in place; and being structured in a hybrid suite that combines cath lab and OR personnel.
Ms. Riley: I’d say the keys are a collegial working relationship between cardiologists and surgeons, and the other specialists involved; having a TAVR coordinator and inpatient NP in place; and being structured in a hybrid suite that combines cath lab and OR personnel.
Ms. Fowler: The hospital administration’s support has been critical. These programs don’t just come out of thin air — you have to have capital involvement and a marketing department to make your program known locally and nationally.
Ms. Ledbetter: We’ve really focused on that multidisciplinary team approach, and blending the OR and the cath lab, with the ICU in the background to take care of these walking critical care patients. If one domino on the continuum falls, things can go the wrong way for these patients. Everybody involved in our program — the hospital administration, the in-house staff, the independent physicians — takes a patient-centered team approach.
