


Smartphones and STEMIs
It’s 1 am and my beeper goes off. The readout says, “STEMI in ED, bed 5.” I have a beeper (read “pager”) — an old-fashioned, on my belt, gray button beeper. I carry the STEMI beeper because our paging system cannot reach all places where our cell phones should work (like the basement of the VA hospital). In the days before I had my smartphone, I might have done one of three things: 1) jump in my car and head to the hospital, trusting the accuracy of the emergency department to read a STEMI ECG; 2) call the ED, ask to speak to the doctor in charge of the patient, and get his description of the ECG and the patient, trusting he could read a STEMI ECG; or 3) fall asleep while waiting for a fax of the ECG to my house, then awake at the second STEMI page and ultimately, go to the hospital, fax available or not.
“pager”) — an old-fashioned, on my belt, gray button beeper. I carry the STEMI beeper because our paging system cannot reach all places where our cell phones should work (like the basement of the VA hospital). In the days before I had my smartphone, I might have done one of three things: 1) jump in my car and head to the hospital, trusting the accuracy of the emergency department to read a STEMI ECG; 2) call the ED, ask to speak to the doctor in charge of the patient, and get his description of the ECG and the patient, trusting he could read a STEMI ECG; or 3) fall asleep while waiting for a fax of the ECG to my house, then awake at the second STEMI page and ultimately, go to the hospital, fax available or not.
With the sensitivity of our cath lab and ED to meeting the goals of the door-to-balloon time (D2B) initiative, my experience, and probably that of many other cardiologists, is that about 25-30% of STEMI pages turn out to be false activations due to an error of the computer readout on the ECG, artifact in transmission from the ambulance in the field, or abnormality on the ECG which is not a true STEMI, but is interpreted as one by a paramedic or the ED doctor. In our system, the cardiology fellow usually beats me to the hospital, reviews the patient and the ECG, and confirms or cancels the STEMI team call-in. On occasion, the cardiology fellow asks for help from the attending before cancelling the STEMI.
Fast forward to our current era of smartphones with image, texting, and internet/ email capabilities. All of the cardiology attendings, fellows, most nurses, and ED and cath lab staff have one. With the smartphones, the workflow for the cath lab STEMI emergency has dramatically changed.
The STEMI story
Let’s look at our most recent case. On Sunday morning at about 10 am, the ED activated the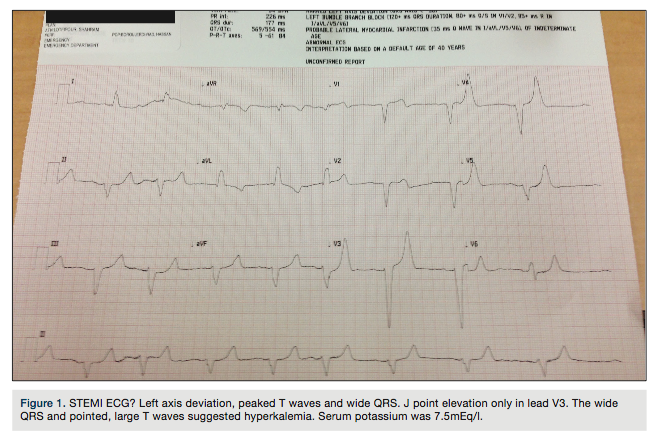 STEMI team for a 61-year-old patient with chest pain for several days, culminating in a prolonged episode. The patient had multiple risk factors for coronary artery disease, peripheral vascular disease, and was on renal dialysis, with the last session 3 days ago. The ECG showed a new left bundle branch block and ischemic T waves (Figure 1), which was new compared to a prior ECG (Figure 2). Compared to only a couple years ago, the scenario leading to decision time is now much abbreviated; hence, I call the ED and ask that the ECG get sent to my phone after speaking to the ED doctor. At the same time, the fellow who was already on-site in the ED sent me a text (Figure 3) for my confirmation. The ECG is peculiar, in that the shape of the T wave in this patient having recent dialysis is highly consistent with hyperkalemia. I requested confirmatory ‘stat’ potassium before coming into the hospital. Within 15 minutes, the serum potassium was found to be 7.5mEq/l (normal 3.5-5.0 mEq/l). With the chest pain controlled with nitroglycerin and antihypertensives, the STEMI was cancelled and the team was turned
STEMI team for a 61-year-old patient with chest pain for several days, culminating in a prolonged episode. The patient had multiple risk factors for coronary artery disease, peripheral vascular disease, and was on renal dialysis, with the last session 3 days ago. The ECG showed a new left bundle branch block and ischemic T waves (Figure 1), which was new compared to a prior ECG (Figure 2). Compared to only a couple years ago, the scenario leading to decision time is now much abbreviated; hence, I call the ED and ask that the ECG get sent to my phone after speaking to the ED doctor. At the same time, the fellow who was already on-site in the ED sent me a text (Figure 3) for my confirmation. The ECG is peculiar, in that the shape of the T wave in this patient having recent dialysis is highly consistent with hyperkalemia. I requested confirmatory ‘stat’ potassium before coming into the hospital. Within 15 minutes, the serum potassium was found to be 7.5mEq/l (normal 3.5-5.0 mEq/l). With the chest pain controlled with nitroglycerin and antihypertensives, the STEMI was cancelled and the team was turned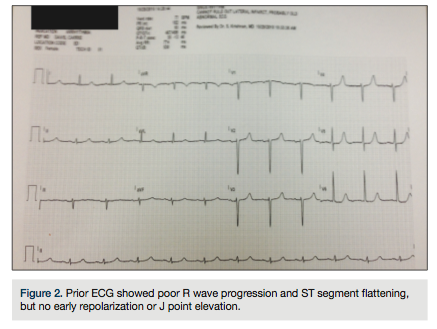 around. The patient was admitted for acute coronary syndrome, but not STEMI.
around. The patient was admitted for acute coronary syndrome, but not STEMI.
The smartphone and STEMI activation
This case illustrates the helpful nature of smartphone communication in the management of the STEMI patient. A STEMI patient that comes in the middle of the night can be correctly triaged while I am still at home. The ED doctor speeds the process by sending a picture of the ECG to me; I can quickly confirm the STEMI without losing too many valuable D2B minutes. After confirmation of the ECG, I’m off to the hospital; or if the ECG produced a false activation, I cancel the STEMI and turn the team around. (My apologies to the cath lab staff, but not all the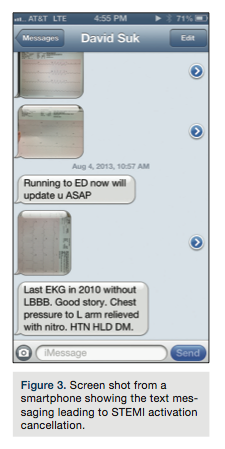 team can stay at home in bed until we confirm the true STEMI, as that might produce the dreaded >90 minutes D2B delay.)
team can stay at home in bed until we confirm the true STEMI, as that might produce the dreaded >90 minutes D2B delay.)
The smartphone has greatly reduced false activations of our STEMI team, an important contribution with both a clinical and economic impact. In addition, the ability of text messaging to rapidly communicate with my fellows facilitates patient care decisions, procedure start times, lunch time meetings, etc., without excess phone calls, dropped calls, and confused verbiage with poor cell phone connections. Many a clever fellow has used their smartphone to take a video of an echocardiogram in order to give me an impression of whether a patient may have tamponade, cardiomyopathy, or significant valve disease. Even a quick image of the patient (with permission) to see a specific physical finding (e.g. ulcerated leg wound) is helpful.
Social media
Smartphones and their connectivity to social media, e.g. Twitter and Facebook, appear to be changing the face (no pun intended) of medical information exchange. The use of social media is rapidly expanding as evidenced by the growth of Facebook users, especially over the age of 50. There are many health care providers that are avid users, and certainly all of us have many friends who are intimately involved with their Facebook friends. I confess that although I know how to use my smartphone, I know almost nothing of how to use Twitter and I’m not on Facebook yet, but not for any special reason other than I’m not sure my friends and family want to hear about my day, every day.
Smartphones and HIPAA
Here’s my cautionary note on smartphone and social media use for medical applications. As with all medical communications, we must be attentive to maintain HIPAA protection. HIPAA issues surrounding the use of any ‘social media’ as it pertains to patient care are just as important as any verbal or written communications. We can never share patient-specific information that may be seen by persons not directly involved in the care of the patient. I do not believe that Twitter communiques will be helpful (yet) because as I understand it, the “Tweet” goes out to all who follow the “Tweeter” and cannot be cancelled. It’s possible that a specific group of people can use Twitter to receive the STEMI activation, but as I learned, the number of followers can be quite large and as they say about Las Vegas, “What you say on Twitter, stays on Twitter,” so be careful.
The same issue likewise applies to other types of social media. While I do not have a Facebook page, many of my colleagues, family and friends find this mode of information exchange wonderfully informative, entertaining, and enlightening, but sometimes frightening. I cringe at some of the less than thoughtful comments, images, and political thought that are transmitted just because the user can do so. As for the medical applications of Facebook, discussions of people with medical illnesses should remain in the “restricted” file in accordance with HIPAA rules or at least the “friend” should use good common sense not to spread information that the afflicted person would not want shared. Like many of my contemporaries, I will need more education on the best uses of social media, but many companies, products, and healthcare groups use Facebook to keep their public informed (Figure 4).
Bottom line
For the cath lab, I think the best communication advance provided by the smartphone, in addition to the STEMI story above, is the use of group text messaging to the cath lab team. This method lets everyone know about timing of procedures, special procedure needs, consents that are missing, labs that need checking, etc., all before the patient arrives in the lab. I’m sure this is not news, but the widespread applicability and presence of the smartphone among my cath lab team has made this approach a reality as both a time saver and patient care enhancer.
At the SCAI 2014 annual meeting in Las Vegas, May 25-28, 2014, we are planning to use smartphones and social media to enhance attendees’ educational experience with participation through smartphone application polling, Twitter interaction with the presentations for questions, and access to experts over the meeting for information. Twitter will announce the hottest sessions and current activities so that those interested can attend something they might have missed without such updates.
I just got my Twitter account set up with the help of my daughter. The looks she gave me as I stumbled through the set up and learning about “@” and “#”, made me laugh as I experienced a reversal of life roles — she, the teacher and me, the student. Many of us will have to be schooled anew on using modern technology. To make the most out of communication, we all just have to dive in and start swimming.
