


Should You Do a Radial Artery Cath in Patients Needing CABG or Dialysis?
With contributions from Drs. Peter Verlee, Will Suh, Aaron Kaplan, John Bittl, Ken Rosenfield, Lloyd Klein, Bonnie Weiner, and John Hirshfeld.
 Practical questions from my colleagues are the source of valuable information for all of us working in the cath lab. Recently, Dr. Peter Verlee, from Maine, had a dilemma. “One of our cardiac surgeons asked me a question. A patient was referred to him for CABG and he wanted to use the radial artery from the left (non-dominant) arm because the patient had poor quality veins. The patient had had a radial cath through that (left) side. I am not sure of the reasons the cardiologist used the left radial artery, but we occasionally use the left side for short people, patients with bypass grafts, or problems with the right radial circulation.
Practical questions from my colleagues are the source of valuable information for all of us working in the cath lab. Recently, Dr. Peter Verlee, from Maine, had a dilemma. “One of our cardiac surgeons asked me a question. A patient was referred to him for CABG and he wanted to use the radial artery from the left (non-dominant) arm because the patient had poor quality veins. The patient had had a radial cath through that (left) side. I am not sure of the reasons the cardiologist used the left radial artery, but we occasionally use the left side for short people, patients with bypass grafts, or problems with the right radial circulation.
“My question is, will there be any problems using the radial as a graft soon after a cath? I told him if the artery was small, I’d be worried about it. If it was of good size, there was probably little danger in using it, and little chance we did anything to injure it during the cath. But I don’t really know. We always use a radial cocktail of nitro and verapamil intra-arterial and IV heparin 50/kg as a bolus routinely. We use 5F catheters and always exchange over a wire. I’m wondering about the use of a radial artery as a conduit within a few days or weeks of a cath.
“As a second and correlative question, do you perform radial access in a patient with a dialysis fistula on the opposite side?”
I sent the questions to my colleagues and received some great responses. First, here’s what I said. If a surgeon told me in advance he was using the radial artery for a conduit, I would not use it and would select an alternate access route. Data in support of this, to my knowledge, is sparse. I know there are studies on radial artery injury after radial cath and so I would extend the inferences from these studies that there is at least local puncture site injury (and as an aside, may be a reason for silent artery closure). The same reasoning to avoid the radial artery would apply for dialysis patients who will likely need another arm for a fistula in future.
Dr. Will Suh, from UCLA, responded, “A paper by Yonetsu et al1 demonstrated by optical coherence tomography that there are acute intimal tears and chronic intimal thickening associated with transradial catheterization. [MK: I wanted to share more details from Dr. Yonsetu’s study. Transradial coronary intervention (TRI) may introduce trauma to the radial artery (RA), and possibly influence quality as a bypass conduit if subsequently used. Yonetsu et al determined the acute and chronic effects of TRI on the RA by optical coherence tomography (OCT) in 73 RAs (in 69 patients). The sheath was pulled back 2 cm distal to the puncture site, and OCT imaging was performed. The acute injuries and intimal thickening were compared between first-TRI RAs and repeat-TRI RAs. Intimal tears were observed in 49 RAs (67.1%) and were more frequent in the distal than in the proximal RA (P = 0.001). Medial dissections were not uncommon (26 RAs, 35.6%). The frequency of acute injury was significantly higher in repeat-TRI RAs (P < 0.001). Intima/medial area, the maximum intimal thickness/medial thickness ratio, and percent narrowing were all significantly greater in repeat-TRI RAs in the distal and proximal RA. Significant acute injuries and chronic intimal thickening of the RA occurs after TRI. It is unknown whether this will impact on long-term graft patency and on clinical outcomes after bypass surgery.] For this reason, I believe a radial artery that has been used as access site for radial cath should be avoided (for CABG) unless it is the only remaining conduit. As for the dialysis patient, I have not avoided radial cath since the injury is primarily distal and a future AV graft would usually be placed more proximally in the arm.”
I looked online to see additional comments. From the Transradial University website (https://www.transradialuniversity.com/faqs), Dr. John T. Coppola, NYU Langone Medical Center, reports “In a paper our group published, we found post-procedural evidence of increased inflammatory cells and vascular damage in the radial artery used to gain access for the catheterization procedure. At the time of surgery, the contralateral or ipsilateral radial artery was harvested for bypass use. At that time, a tissue specimen was provided for histological examination, whereupon it was noted there was visual evidence of vascular disease. This may be why the radial artery is not such a great conduit for a bypass graft. If the radial artery is expected to be used for bypass, then the contralateral radial artery should be utilized for catheterization.”
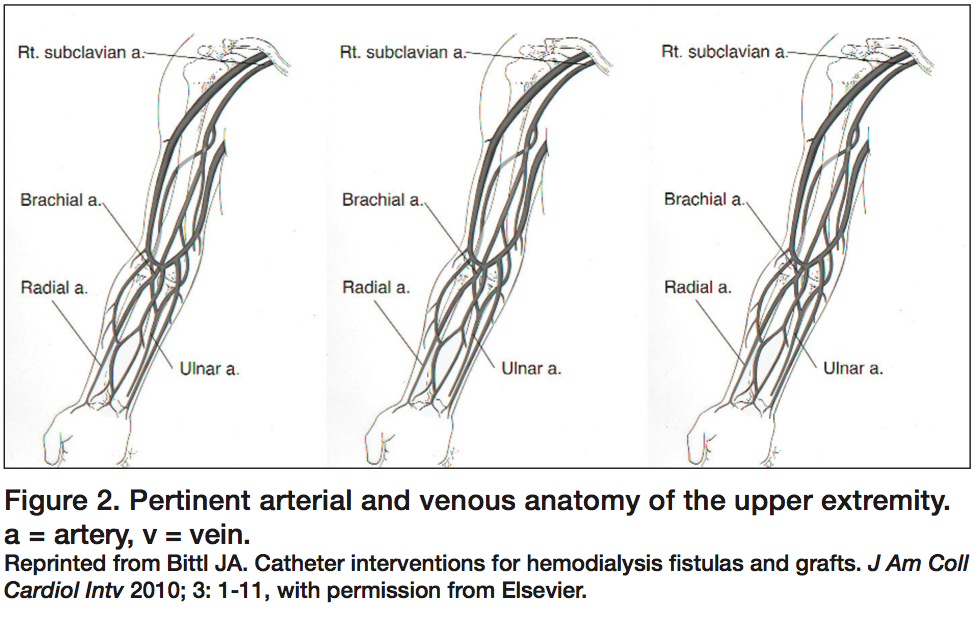
 Dr. John Bittl, from Ocala, Florida, commented, “I wouldn’t recommend the use of the radial approach in either side in a patient who needs hemodialysis access creation. Although the K/DOQI (Kidney Disease Outcomes and Quality Intitiative) guidelines contain no statement against using a transradial approach for cardiac catheterization2, our nephrologists state that the need for hemodialysis access creation is a strong contraindication against a transradial catheterization and recommend a transfemoral approach whenever possible. It is important to remember that only 20% to 40% of radial-cephalic fistulas mature adequately for hemodialysis under the best circumstances.3,4 Prior trauma from venipunctures (or arterial punctures) at any time is stated to reduce the chance of future success of autogenous arteriovenous access maturation in either the dominant or nondominant arm, and most patients on hemodialysis ultimately require accesses creation in multiple sites because of the finite patency of fistulas and grafts.2 In a patient who has undergone a recent transradial catheterization and needs dialysis access creation, I would try to find a vascular surgeon who has good success with transposed brachial-basilic fistulas” (See Figures 1-2).
Dr. John Bittl, from Ocala, Florida, commented, “I wouldn’t recommend the use of the radial approach in either side in a patient who needs hemodialysis access creation. Although the K/DOQI (Kidney Disease Outcomes and Quality Intitiative) guidelines contain no statement against using a transradial approach for cardiac catheterization2, our nephrologists state that the need for hemodialysis access creation is a strong contraindication against a transradial catheterization and recommend a transfemoral approach whenever possible. It is important to remember that only 20% to 40% of radial-cephalic fistulas mature adequately for hemodialysis under the best circumstances.3,4 Prior trauma from venipunctures (or arterial punctures) at any time is stated to reduce the chance of future success of autogenous arteriovenous access maturation in either the dominant or nondominant arm, and most patients on hemodialysis ultimately require accesses creation in multiple sites because of the finite patency of fistulas and grafts.2 In a patient who has undergone a recent transradial catheterization and needs dialysis access creation, I would try to find a vascular surgeon who has good success with transposed brachial-basilic fistulas” (See Figures 1-2).
 Another point from the Transradial University website (from https://www.transradialuniversity.com/faqs) was from Dr. Sandeep Nathan, University of Chicago Medical Center. He states, “Based on the prospectively collected registry data at our institution, post-procedural radial artery occlusion at 6-24 hours is < 1%. It should be noted that we routinely use an anticoagulant/spasmolytic cocktail in all patients, immediately following sheath insertion and this may impact patency rates (vs. selective use). In other published literature, the rate of spontaneous radial recanalization has been estimated at 50-70%. In discussions with our vascular surgery colleagues, it seems unlikely that radial access would compromise dialysis access in the future.”
Another point from the Transradial University website (from https://www.transradialuniversity.com/faqs) was from Dr. Sandeep Nathan, University of Chicago Medical Center. He states, “Based on the prospectively collected registry data at our institution, post-procedural radial artery occlusion at 6-24 hours is < 1%. It should be noted that we routinely use an anticoagulant/spasmolytic cocktail in all patients, immediately following sheath insertion and this may impact patency rates (vs. selective use). In other published literature, the rate of spontaneous radial recanalization has been estimated at 50-70%. In discussions with our vascular surgery colleagues, it seems unlikely that radial access would compromise dialysis access in the future.”
Dr. Aaron V. Kaplan, from Lebanon, New Hampshire, replied, “I agree and would avoid radial approach when there is a high likelihood it might be used as a graft conduit. The robustness of the radial approach is based on that it is a very forgiving artery, i.e., flow-limiting injury is typically sub-clinical. This is because the radial artery is not an end artery and that the downstream O2 demands are minimal (i. e. there is not much muscle mass in the hand) and can easily be handled by the ulnar artery. We know that radial artery removal for CABG is well tolerated. The subclinical injury should not be confused with no injury which may be important when the radial artery is perfusing tissue in a supra- or extra-physiologic fashion, e.g., CABG conduit and also dialysis. We know that radial artery access frequently injures the artery and that radial artery occlusion, when looked for in a systematic fashion, is frequent.5 I also agree that there are no real outcomes data to drive this decision.”
Dr. Ken Rosenfield, from Boston, Massachusetts, adds, “I was going to agree with all comments so far in that the use of an instrumented radial for bypass conduit should be avoided [especially if the studies of radial injury are accurate]. I like radial access, but sometimes I think some of us have drunk too much of the ‘radial Kool-Aid’.”
Dr. Bonnie Weiner from Worchester, Massachusetts, said, “As a non-radial evangelist (and being old) I hear the same arguments for radial access as I heard 30 years ago by the Sones evangelists. Yes, much has changed, but much has also stayed the same. It is also important to recognize that the complication rate for femoral access (the major motivator for alternative access) has gone down dramatically. The differential between the two approaches is therefore diminishing anyway. We also need to maintain our femoral access skills and teach our fellows how to do that well, particularly as our cases become more complex. That having been said, I also share the concern about the future need for radial conduits for CABG. No, there is not a huge amount of science about the value of radial grafts for bypass, but there is enough for good surgeons to want to use as much arterial conduit as they can. We should not be discouraging that, or limiting the options just because it is ‘in’ to do radial procedures.”
Dr. John Hirshfeld, from Philadelphia, Pennsylvania, notes, “I have been concerned about the issue of radial artery injury from the very beginning of radial access popularity. I agree that if we really work at controlling femoral access complications, we should do a good deal better than what is published in clinical trials. It seems to me that there is no way that an artery like the radial is not transformed by being instrumented by a catheter that is close to its native diameter. In addition, as is the case with restenosis, the smaller the artery, the less neointimal hyperplasia it can tolerate. While one can get away with losing it as a consequence of a procedure, the loss of it as a potential future revascularization conduit could be detrimental down the road.”
Dr. Lloyd Klein, from Chicago, Illinois, said, “Although it seems intuitive that acute injury will be inevitable, this does not necessarily translate into permanent damage, assuming the injuries are not frank complications. But the necessity for actual data is apparent. I wouldn’t do a procedure through the radial if I knew it was going to be used for dialysis, but if a procedure had been done in the recent or distant past, it should not preclude its use.
“I still do plenty of percutaneous brachial catheterizations and percutaneous coronary interventions in patients who have problematic access via femoral approach, although such cases are much fewer compared to the past, because the femoral technique has improved [so much] over these past 20 years. I see no reason to learn radial when brachial works just fine. There are more complications with brachial or radial than femoral, but that too could be a function of case selection. If it is routinely done by that technique in every case, probably the overall incidence of problems is similar. [MK: I guess you and Bonnie don’t like radial cath that much. That’s OK, too, and thanks for the input viewed from the femoral approach].
“I echo John Hirshfeld’s concerns about radial access. I just think we need some real data on the subject.”
I am sure we can still find a spectrum of opinion on use of the radial for future CABG and dialysis patients. I believe all agree that we should carefully assess in whom and when radial access should be avoided. The bottom line from my colleagues’ comments above is that at least for now and in the near future with the information available, if your patient’s radial artery will be needed for surgery or dialysis, it is best to preserve this vessel and pick another access.
References
- Yonetsu T, Kakuta T, Lee T, Takayama K, et al. Assessment of acute injuries and chronic intimal thickening of the radial artery after transradial coronary intervention by optical coherence tomography. Eur Heart J 2010 Jul; 31(13): 1608-1615. Epub 2010 Apr 22.
- Vascular Access 2006 Work Group. NKF-DOQI clinical practice guidelines for vascular access, update 2006. Am J Kidney Dis 2006; 48(Suppl 1): S176-S306.
- Dember LM, Beck GJ, Allon M, et al. Effect of clopidogrel on early failure of arteriovenous fistulas for hemodialysis: a randomized controlled trial. JAMA 2008; 299: 2164-2171.
- Dixon BS, Beck GJ, Vazquez MA, et al. Effect of dipyridamole plus aspirin on hemodialysis graft patency. N Engl J Med 2009; 360: 2191-2201.
- Uhlemann M, Möbius-Winkler S, Mende M, Eitel I, et al. The Leipzig prospective vascular ultrasound registry in radial artery catheterization: impact of sheath size on vascular complications. J Am Coll Cardiol Intv 2012; 5(1): 36-43.
Disclosure: Dr. Kern reports that he is a speaker for Volcano Therapeutics and St. Jude Medical, and is a consultant for Merit Medical.
