


Your Path to Success: Expert Advice
Revenue Analysis of Hospital-Based Vs. Physician Office Non-Invasive Diagnostic Testing
Editor's Note: This article has been corrected from the print version. Table 1 has been corrected.
Now, more than ever, hospital-physician alignment and integration are at the forefront of discussion in the healthcare industry. As Corazon works with all types of organizations across the country, we find this topic to be “hot” on the minds of hospital leaders and physicians alike. Hospitals are interested in working with physicians in order to prepare for the imminent uncertainty of healthcare reform, while physicians are interested in opportunities with hospitals as a means to ensure future financial viability as the threat of reimbursement cuts continue.
Physicians in particular felt the threat of declining reimbursement when their payments were expected to decline approximately 25% as part of the proposed Physician Fee Schedule (PFS) and Sustainable Growth Rate (SGR) formula, with non-invasive diagnostic cardiology testing as one of the hardest-hit physician procedures. During a tumultuous 2010, the anticipated loss in physician revenue, coupled with the most utilized office-based cardiology test, would no longer be enough to financially sustain most current practice models.
Although the projected decreases did not occur in 2010 or 2011, they are once again scheduled for 2012. In order to remedy looming reductions, cardiology practices continue to approach hospitals with alignment strategies, particularly related to the conversion of office-based non-invasive cardiology testing into outpatient departments of the hospital. This model creates the opportunity for physicians to “sell” the business to the hospital and mitigate any future revenue risks, while the hospital gains additional non-invasive volume at hospital reimbursement rates.
Understanding the conversion of office-based to hospital-based and the reasons why hospital administration and physicians are interested are necessary in order to competently address the issue.
discussion in the healthcare industry. As Corazon works with all types of organizations across the country, we find this topic to be “hot” on the minds of hospital leaders and physicians alike. Hospitals are interested in working with physicians in order to prepare for the imminent uncertainty of healthcare reform, while physicians are interested in opportunities with hospitals as a means to ensure future financial viability as the threat of reimbursement cuts continue.
Physicians in particular felt the threat of declining reimbursement when their payments were expected to decline approximately 25% as part of the proposed Physician Fee Schedule (PFS) and Sustainable Growth Rate (SGR) formula, with non-invasive diagnostic cardiology testing as one of the hardest-hit physician procedures. During a tumultuous 2010, the anticipated loss in physician revenue, coupled with the most utilized office-based cardiology test, would no longer be enough to financially sustain most current practice models.
Although the projected decreases did not occur in 2010 or 2011, they are once again scheduled for 2012. In order to remedy looming reductions, cardiology practices continue to approach hospitals with alignment strategies, particularly related to the conversion of office-based non-invasive cardiology testing into outpatient departments of the hospital. This model creates the opportunity for physicians to “sell” the business to the hospital and mitigate any future revenue risks, while the hospital gains additional non-invasive volume at hospital reimbursement rates.
Understanding the conversion of office-based to hospital-based and the reasons why hospital administration and physicians are interested are necessary in order to competently address the issue.
What Does this “Conversion” Mean?
Essentially, if a private cardiology practice is interested in converting the office-based testing to a hospital-based provider, then the hospital must “purchase” that book of business from the practice at a fair market value price. Before the “purchase,” both parties must first evaluate whether the office-based testing location will meet the Centers for Medicare and Medicaid (CMS) criteria to become hospital-based. A selection of requirements includes:- Ownership: Off-campus location can only be provider-based if they are 100% owned by the main provider (i.e., the hospital).
- Administration and Supervision: Main provider has the same level of accountability and reporting relationships as it does with its existing departments.
- Location: Off-campus location must be within 35 miles of hospital campus (there are some exceptions).
- Notice to Patients: Must provide written notice that the patient will incur a coinsurance liability to the hospital that he or she would not have incurred previously, in addition to an Advanced Beneficiary Notification (ABN) for non-covered services.
- Staff: Main provider must employ the staff that is directly involved in patient care. The hospital is not required to employ the physicians or physician assistants.
- License: Off-campus location must operate under the same license as main provider.
- Clinical Services:
- Professional staff has privileges at main provider.
- Main provider maintains oversight of the facility as it does for any other department of the main provider.
- Medical director of the off-campus location reports to Chief Medical Officer of the main provider.
- Medical staff committees at the main provider are responsible for the medical activities at the off-campus location.
- Medical records are integrated or cross-referenced to the main provider records.
- Financial Integration: Financial operations are integrated into main provider’s financial system. The off-campus location must be reported as a cost center of the main provider.
- Public Awareness: Off-campus location must be clearly identified as part of the main provider (e.g., shared name, patient registration forms, letterhead, signage, website, etc.).
Why “Convert” to Hospital-Based?
The most significant difference between office-based and hospital-based non-invasive testing is the estimated technical reimbursement associated with the procedures.- If the office can be converted to an outpatient department of the hospital, then the hospital is able to bill the technical fee for the procedures using the hospital outpatient ambulatory payment classification (APC) structure.
- If the office cannot be converted to hospital-based, then the physician will continue to bill the technical fee using the physician fee schedule.
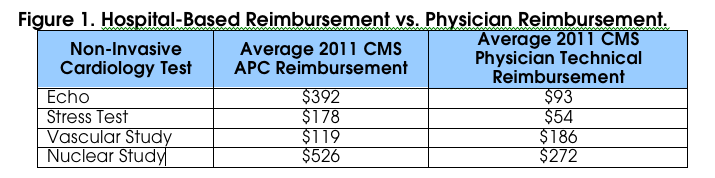 as illustrated in Table 1.
The reason payment is different for hospital-based services is because payment assumes additional overhead and higher expenses related to operating a hospital, such as inpatient care, ancillary departments, facility maintenance, housekeeping, dietary, and so on. Whereas in a practice setting, overhead and expenses tend to be lower due to differences in staffing ratios, employee benefits, and outpatient care.
as illustrated in Table 1.
The reason payment is different for hospital-based services is because payment assumes additional overhead and higher expenses related to operating a hospital, such as inpatient care, ancillary departments, facility maintenance, housekeeping, dietary, and so on. Whereas in a practice setting, overhead and expenses tend to be lower due to differences in staffing ratios, employee benefits, and outpatient care.
Case Study
We have aided multiple organizations nationwide in the education and facilitation of hospital-physician alignment and integration, with particular focus on the financial revenue comparison of office-based versus hospital-based non-invasive diagnostic testing. This is particularly important, because understanding the revenue differential, even in light of the costs associated with a change in status, is essential to understanding the impact of implementing a new model. One New Jersey facility utilized Corazon to develop an alignment strategy between the hospital and a closely affiliated private practice cardiology group. The engagement included an educational session focusing on current industry models, the facilitation of alignment discussions, a financial analysis for hospital-based reimbursement, and recommendations for next steps. The private cardiology practice interested in aligning with the hospital consisted of 7 cardiologists (6 non-invasive cardiologists and 1 interventional cardiologist) with an office-based non-invasive cardiology procedure volume of approximately 5,500 cases per year. Both parties were interested in exploring alignment models that could strengthen their commitment, better align goals for patient care excellence, support program development, and ensure financial viability. Corazon utilized detailed data received from the hospital and the practice including volume by CPT code, payor mix, reimbursement, and other associated data. Without the cooperation and willingness of the cardiology practice to share confidential information, Corazon, nor any other organization or individual for that matter, would not have been able to accurately complete the analysis. We applied the client-specific payor mix and reimbursement assumptions to calculate the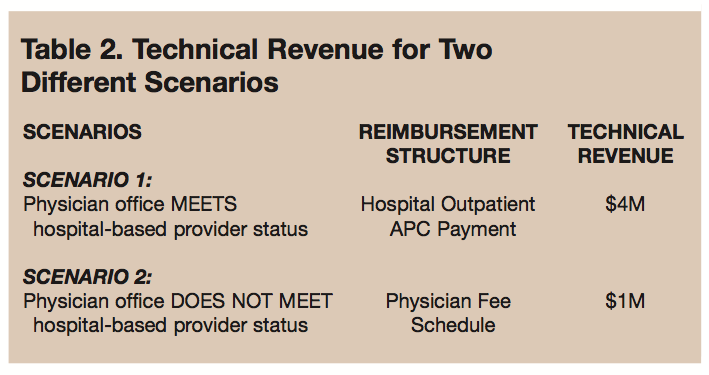 technical revenue for two scenarios, as illustrated in Table 2. The difference in technical revenue for 5,500 non-invasive procedures was approximately $3,000,000.
technical revenue for two scenarios, as illustrated in Table 2. The difference in technical revenue for 5,500 non-invasive procedures was approximately $3,000,000.
Recommendations and Conclusion
Converting from a physician office to a hospital-based provider is certainly not an easy task to achieve. There are multiple risks and considerations that must be well thought out, and both the hospital and the practice must complete their due diligence related to all facets of the change. When approaching alignment, we advise contracting with an outside third party to:- Present an alignment educational session to the hospital and key cardiology groups as a means to facilitate discussion.
- Conduct separate meetings with the hospital and key cardiology groups to solicit candid opinions and needs for an alignment.
- Evaluate various alignment models that identify opportunities to benefit both the hospital and the cardiology group.
- Project a financial analysis for the selected alignment model.
- Develop a work plan for implementation outlining suggesting timeframes and responsible parties.
Reference
- Provider-based Status On or After October 1, 2002. Centers for Medicare and Medicaid Services. Full CMS criteria is available for download at: https://www.cms.gov/ transmittals/downloads/A03030.pdf. Accessed January 24, 2011.
 Kristin is a Consultant at Corazon, Inc., offering a full continuum of services in heart, vascular, and neuro specialties, including consulting, recruitment, and interim management. To learn more, visit www.corazoninc.com, or call (412) 364-8200. To reach Kristin, email ktruesdell@corazoninc.com
Kristin is a Consultant at Corazon, Inc., offering a full continuum of services in heart, vascular, and neuro specialties, including consulting, recruitment, and interim management. To learn more, visit www.corazoninc.com, or call (412) 364-8200. To reach Kristin, email ktruesdell@corazoninc.com
