


Reducing Operating Costs While Increasing Quality
This article is reprinted with permission from Medical Construction and Design July/August 2011: 46-48. In this era of health care and financial reform, hospital officials are turning to measures that promise to reduce costs yet still improve the quality of care. Consolidating a hospital’s surgical and catheterization departments not only promises those benefits, but will absolutely deliver them — as long as the consolidation process includes strategic changes in staffing and operational management.
In this era of health care and financial reform, hospital officials are turning to measures that promise to reduce costs yet still improve the quality of care. Consolidating a hospital’s surgical and catheterization departments not only promises those benefits, but will absolutely deliver them — as long as the consolidation process includes strategic changes in staffing and operational management.
The architectural design process required to consolidate two departments in a new hospital is reasonably clear. Consolidating the departments in an existing hospital, however, can be more complex.
The real challenges involve staffing and operational management. Physicians and staff often resist consolidation. The smaller group worries about a loss of autonomy. The larger department believes the change will increase crowding. While these concerns have some validity, the benefits of consolidation far surpass the hurdles.
Managed properly, consolidation delegates tasks such as inventory management, material handling, scheduling and other clerical tasks to appropriate personnel. As a result, nurses and others charged with supporting surgical and catheterization procedures can be cross-trained to focus more on patient-care tasks that are more in line with their professional interests.
Procedures then go more smoothly for physicians and nurses. Often, the reorganization can provide efficiencies that allow staff to be more productive. Increased productivity, of course, also benefits the hospital’s profit and loss statement as well as quality of care.
Consolidating space in a replacement hospital
 Consolidating surgical and catheterization units in a replacement hospital design calls for an architect to innovate the most efficient use of space.
Consolidating surgical and catheterization units in a replacement hospital design calls for an architect to innovate the most efficient use of space.
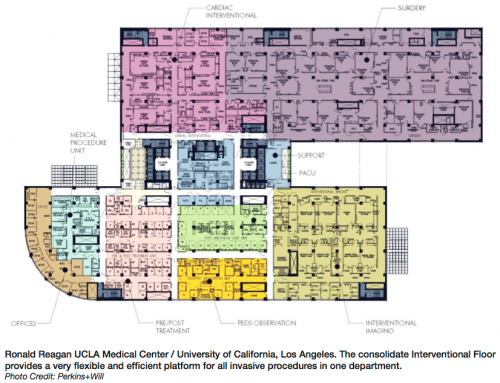
The replacement hospital constructed recently at the UCLA Medical Center in Los Angeles is an example. Here, the modularity of the procedure rooms allows for easy change, including more control rooms required for catheterization procedures.
The total aggregate floor area is substantially less than providing the program needs in two or three separate departments.
Additionally, the consolidated replacement hospital needed space and furnishings for only one waiting room, but a larger one and furnished in a way that makes family and friends more comfortable.
Analyzing renovation challenges
The process of consolidating by way of renovation begins with an analysis of the existing floor plans.
Sometimes floor plan adjacencies of functions identifies a surgery department hemmed in by spaces that would prove too costly to move — like a cafeteria with heavy kitchen equipment on one side and radiology on the other.
In many cases, however, a department can expand in one direction, adding operating rooms or cath labs. Often too, the consolidated locker rooms and waiting rooms can go on the floors above or below the department.
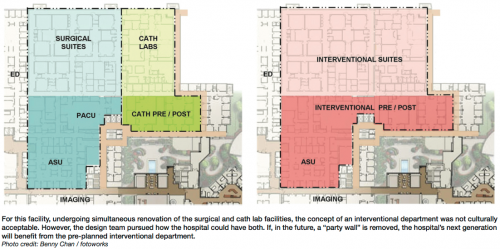
The Swedish American Health System in Rockford, Illinois, recently renovated its facility with an eye toward consolidating its surgical suites with its cath lab units. The project appeared remarkably simple, thanks to an original design that located the departments adjacent to each other, separated only by a public corridor that could be relocated.
The administration authorized a partial renovation that would make eventual full consolidation quick and easy, demonstrating the cost and quality of care benefits of additional aspects to staff.
The partial renovation transformed the public corridor into an internal corridor for the surgical department, replacing the wall enclosing the cath labs with an easily removed party wall. The renovation treated recovery space in a similar fashion, placing each set of recovery rooms adjacent to the other with a removable wall in between.
Benefiting the staff
Ensuring that consolidation will benefit the physicians and the hospital is a more central undertaking. That task begins with demonstrating to the physicians and staffs in the surgery and cardiology, as well as interventional radiology departments, that consolidation will make their lives easier, to the extent that they engage the endeavor.
The cardiologists from the catheterization group and the physicians who work in the surgical suites will likely have different concerns. Because cardiologists do not compete with other departments for cath lab time, they often grow accustomed to scheduling at their convenience. Consolidation, they are likely to believe, will change that. On the flip side, surgeons would probably prefer not to add another group to those already competing for limited OR space.
But consolidation solves both of these problems for physicians and brings other benefits, many related to costs, to the hospital.
While consolidation can reduce the overall number of procedure rooms, the square footage devoted to the pre- and post-procedure area, and the space required for locker rooms, it will also provide more OR, support, and locker room space than either surgeons or cardiologists had access to before consolidation.
An analysis of previous use of the cath lab, OR suites and support space can ensure that consolidation will produce facilities adequate to the work and perhaps even allow for growth, while making excess square footage available for other hospital uses.
In addition, the consolidated department obtains access to the more professional scheduling capabilities generally available when staffing larger departments. Greater volume schedulers understand the need to start on time and finish as close to the scheduled finishing time as possible. They handle insurance requirements ahead of time, ensure that pre-admission procedures are carried out, schedule and notify pre- and post-procedure staff, and generally make sure that everyone knows when and where to be.
Boosting operational efficiency
 Physicians who have elected to engage consolidation generally like the way it helps to organize their time and add to forms of collaboration.
Physicians who have elected to engage consolidation generally like the way it helps to organize their time and add to forms of collaboration.
But that is just the first of the benefits that successful consolidation can deliver to a hospital. Consolidation makes it possible to streamline inventories, improve material handling, and free up existing staff to take on other underserved responsibilities.
A consolidated department can afford its own on-site purchasing and inventory manager. Typically, nurses manage operating room and cath lab inventories, a job for which they are not trained and which takes them away from what they are good at — nursing.
A skilled purchasing manager, on the other hand, collaborates with the hospital’s main purchasing staff, coordinates spending, and gains volume discounts more often.
Consolidating OR, IR and cath-lab units reduces staffing needs. For an overworked nursing staff, consolidation can rationalize schedules and provide relief. In most cases, especially end-of-day staffing such as in recovery, consolidation will free up staff to handle other duties.
The final challenge of consolidating two staffs lies in cross-training, with OR nurses learning cardio procedures and cardio nurses learning OR procedures. Of course, such changes often spark resistance at first. But nurses that have gone through cross training eventually realize that acquiring new skills makes them more capable and more productive.
And that is the overall effect — and goal — of consolidation. It raises the quality of care that the new department is capable of delivering while driving down the cost of that care.
Dennis L. Kaiser, AIA, LEED® AP, Principal, Market Sector Leader, can be reached at (617) 406-3433 or dennis.kaiser@perkinswill.com.
