


Recurrent Stent Thrombosis in a Patient Found to Have Antiphospholipid Syndrome
Abstract
A 53-year-old male presented with unstable angina and was found to have severe coronary artery disease. However, despite percutaneous coronary intervention with adequate anticoagulation, the patient had recurrent stent thromboses during the hospitalization, eventually attributed to antiphospholipid antibody syndrome.
Case
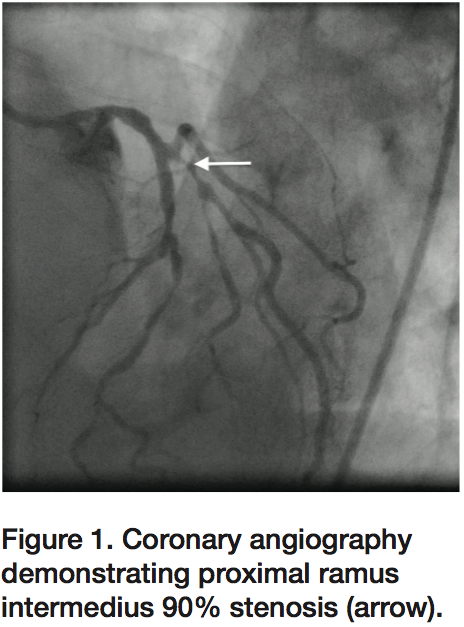 A 53-year-old male with history of paroxysmal atrial fibrillation and inflammatory bowel disease presented with symptoms of unstable angina, beginning 2-3 weeks prior to admission. He reported exertional chest pressure associated with diaphoresis and shortness of breath that resolved with rest. Coronary angiography demonstrated left anterior descending (LAD) artery with proximal 80-90% stenosis and large ramus intermedius (RI) with proximal 90% stenosis (Figure 1). Left ventriculography revealed preserved ejection fraction with no
A 53-year-old male with history of paroxysmal atrial fibrillation and inflammatory bowel disease presented with symptoms of unstable angina, beginning 2-3 weeks prior to admission. He reported exertional chest pressure associated with diaphoresis and shortness of breath that resolved with rest. Coronary angiography demonstrated left anterior descending (LAD) artery with proximal 80-90% stenosis and large ramus intermedius (RI) with proximal 90% stenosis (Figure 1). Left ventriculography revealed preserved ejection fraction with no 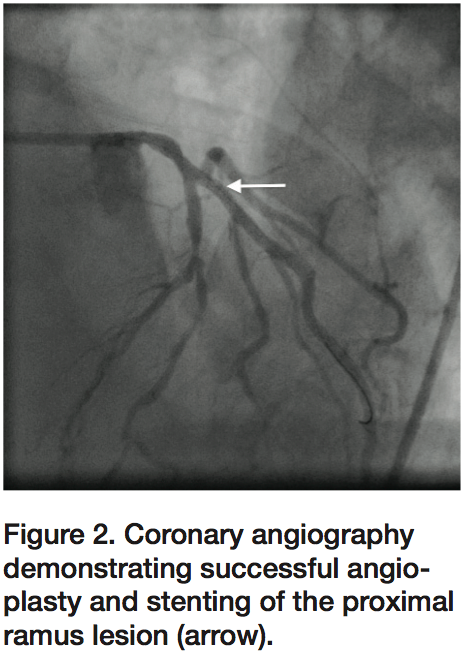 mitral regurgitation. Percutaneous coronary intervention (PCI) was performed in the same setting after anticoagulation using bivalirudin bolus and infusion, and antiplatelet therapy using aspirin 325 mg and clopidogrel 600 mg pre-procedure. The RI lesion was treated with a 2.25 x 24 mm Ion stent (Boston Scientific) and post-dilated using a 2.5 mm non-compliant balloon. Final angiography demonstrated TIMI-3 flow in the RI (Figure 2), and the patient was transferred to recovery in stable condition.
mitral regurgitation. Percutaneous coronary intervention (PCI) was performed in the same setting after anticoagulation using bivalirudin bolus and infusion, and antiplatelet therapy using aspirin 325 mg and clopidogrel 600 mg pre-procedure. The RI lesion was treated with a 2.25 x 24 mm Ion stent (Boston Scientific) and post-dilated using a 2.5 mm non-compliant balloon. Final angiography demonstrated TIMI-3 flow in the RI (Figure 2), and the patient was transferred to recovery in stable condition.
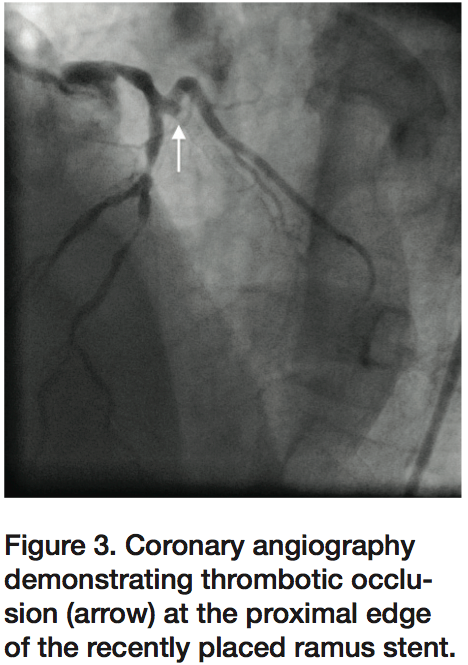 Approximately 25 minutes post-procedure, the patient developed severe chest pressure with lateral ST elevations. The patient was taken back emergently to the catheterization laboratory, where angiography demonstrated 100% thrombotic occlusion of the RI at the proximal edge of the recently placed stent (Figure 3). The patient was re-bolused with bivalirudin, followed by infusion and activated clotting time (ACT) after bivalirudin administration was confirmed to be 397 seconds. Laser atherectomy was performed using a 0.9 mm excimer laser
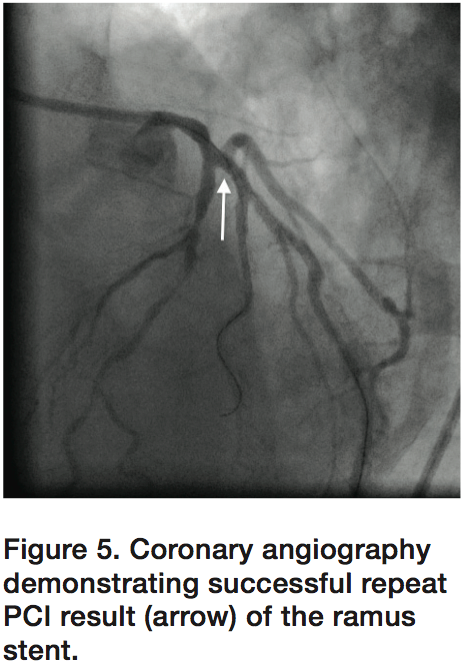
Approximately 25 minutes post-procedure, the patient developed severe chest pressure with lateral ST elevations. The patient was taken back emergently to the catheterization laboratory, where angiography demonstrated 100% thrombotic occlusion of the RI at the proximal edge of the recently placed stent (Figure 3). The patient was re-bolused with bivalirudin, followed by infusion and activated clotting time (ACT) after bivalirudin administration was confirmed to be 397 seconds. Laser atherectomy was performed using a 0.9 mm excimer laser 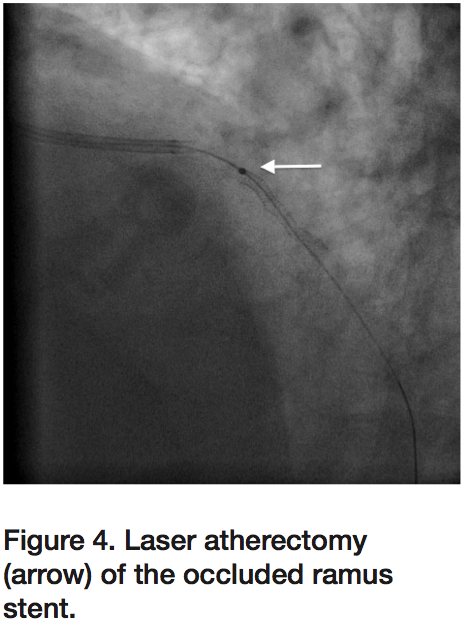 coronary atherectomy catheter (Spectranetics) (Figure 4) with multiple runs, followed by aggressive angioplasty using a 2.75 mm non-compliant balloon and adequate stent expansion confirmed by intravascular ultrasound (IVUS; Boston Scientific). Final angiogram again demonstrated good result with TIMI-3 flow (Figure 5) and resolution of ST changes and chest pressure.
coronary atherectomy catheter (Spectranetics) (Figure 4) with multiple runs, followed by aggressive angioplasty using a 2.75 mm non-compliant balloon and adequate stent expansion confirmed by intravascular ultrasound (IVUS; Boston Scientific). Final angiogram again demonstrated good result with TIMI-3 flow (Figure 5) and resolution of ST changes and chest pressure.
 As the patient was being transferred off the procedure table, he once again developed severe chest pressure and recurrent lateral ST elevations. Angiography again demonstrated 100% thrombotic occlusion of the RI at the proximal edge of the previously placed stent (Figure 6), despite a repeat ACT of 337 seconds. Intravenous eptifibatide was initiated in addition to bivalirudin infusion. Aspiration thrombectomy was performed with multiple passes using an Export catheter followed by IVUS, which again confirmed adequate stent
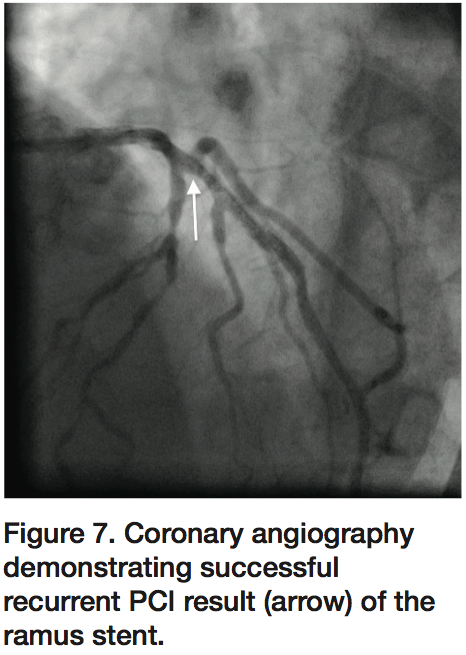
As the patient was being transferred off the procedure table, he once again developed severe chest pressure and recurrent lateral ST elevations. Angiography again demonstrated 100% thrombotic occlusion of the RI at the proximal edge of the previously placed stent (Figure 6), despite a repeat ACT of 337 seconds. Intravenous eptifibatide was initiated in addition to bivalirudin infusion. Aspiration thrombectomy was performed with multiple passes using an Export catheter followed by IVUS, which again confirmed adequate stent 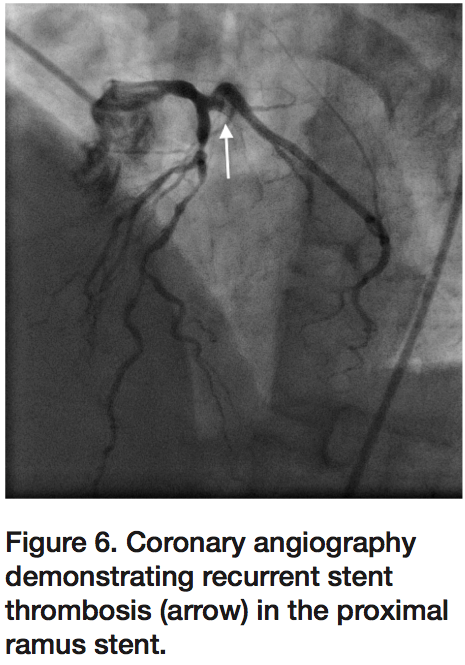 apposition (Figure 7) with good angiographic result and TIMI-3 flow without evidence of dissection or thrombus. The patient’s chest pressure resolved and ST segments normalized, and he was transferred to the ICU with no further episodes of chest pain. Eptifibatide and bivalirudin were continued for 24 hours, and clopidogrel substituted with prasugrel. A hypercoagulable work up eventually demonstrated that the patient was positive for lupus anticoagulant and he was diagnosed with antiphospholipid antibody syndrome (APS). The patient was transitioned to warfarin and discharged home once international normalized ratio (INR) was therapeutic. Discharge medications included aspirin, prasugrel, and warfarin.
apposition (Figure 7) with good angiographic result and TIMI-3 flow without evidence of dissection or thrombus. The patient’s chest pressure resolved and ST segments normalized, and he was transferred to the ICU with no further episodes of chest pain. Eptifibatide and bivalirudin were continued for 24 hours, and clopidogrel substituted with prasugrel. A hypercoagulable work up eventually demonstrated that the patient was positive for lupus anticoagulant and he was diagnosed with antiphospholipid antibody syndrome (APS). The patient was transitioned to warfarin and discharged home once international normalized ratio (INR) was therapeutic. Discharge medications included aspirin, prasugrel, and warfarin.
Discussion
 APS, or antiphospholipid antibody syndrome, is defined by two major components: 1) one or more episodes of venous, arterial, or small vessel thrombosis and/or morbidity with pregnancy, and 2) presence in the plasma of at least one type of autoantibody known as an antiphospholipid antibody on two or more occasions at least 12 weeks apart.1,2 Although the clinical manifestations of APS occur in other disease populations, in APS they occur by definition in the context of antiphospholipid antibodies. APS occurs either as a primary condition (primary APS), or in the setting of an underlying disease (secondary APS). The antiphospholipid antibodies, which are directed against plasma proteins bound to anionic phospholipids, may be detected as: lupus anticoagulants, anticardiolipin antibodies, antibodies to ß2 glycoprotein-I (ß2GPI), or other antibodies, including those to prothrombin, annexin V, phosphatidylserine and phosphatidylinositol. The presence of antiphospholipid antibodies may be demonstrated directly by enzyme-linked immunosorbent assay (ELISA) testing in the case of anticardiolipin antibodies and antibodies to ß2GPI, or by a clotting assay that demonstrates effects of an antiphospholipid antibody on the phospholipid-dependent factors in the coagulation cascade (lupus anticoagulant test).3
APS, or antiphospholipid antibody syndrome, is defined by two major components: 1) one or more episodes of venous, arterial, or small vessel thrombosis and/or morbidity with pregnancy, and 2) presence in the plasma of at least one type of autoantibody known as an antiphospholipid antibody on two or more occasions at least 12 weeks apart.1,2 Although the clinical manifestations of APS occur in other disease populations, in APS they occur by definition in the context of antiphospholipid antibodies. APS occurs either as a primary condition (primary APS), or in the setting of an underlying disease (secondary APS). The antiphospholipid antibodies, which are directed against plasma proteins bound to anionic phospholipids, may be detected as: lupus anticoagulants, anticardiolipin antibodies, antibodies to ß2 glycoprotein-I (ß2GPI), or other antibodies, including those to prothrombin, annexin V, phosphatidylserine and phosphatidylinositol. The presence of antiphospholipid antibodies may be demonstrated directly by enzyme-linked immunosorbent assay (ELISA) testing in the case of anticardiolipin antibodies and antibodies to ß2GPI, or by a clotting assay that demonstrates effects of an antiphospholipid antibody on the phospholipid-dependent factors in the coagulation cascade (lupus anticoagulant test).3
Lupus anticoagulants are antibodies directed against plasma proteins such as ß2GPI, prothrombin, or annexin V that are bound to anionic phospholipids. The term “lupus anticoagulant” is a misnomer for three reasons: 1) the presence of lupus anticoagulants is generally associated with a clotting tendency, not an anticoagulant effect; 2) more than one antibody is associated with lupus anticoagulant activity; and 3) only about 50% of individuals with lupus anticoagulants meet the American College of Rheumatology criteria for the classification of systemic lupus erythematosus (SLE).5 Since there is more than one lupus anticoagulant, and not all antibodies with APS are associated with anticoagulant activity, the detection of lupus anticoagulants occurs through functional clotting tests, and not through ELISAs. Lupus anticoagulants block in vitro assembly of the prothrombinase complex, resulting in a prolongation of in vitro clotting assays. This prolongation is not reversed when the patient’s plasma is diluted 1:1 with normal platelet-free plasma. In contrast, such mixing studies do correct the clotting abnormality associated with factor deficiencies. Although these changes suggest impaired coagulation, patients with lupus anticoagulants have a paradoxical increase in the frequency of arterial and venous thrombotic events.4
The antigens against which the antiphospholipid antibodies are directed and the mechanisms by which antiphospholipid antibodies cause thrombosis are not completely understood. The pathogenesis of the APS-associated clinical manifestations appears to result from a variety of antiphospholipid antibody effects upon pathways of coagulation, including the procoagulant actions of these antibodies upon protein C, annexin V, platelets, serum proteases, toll-like receptors, tissue factor, and via impaired fibrinolysis.5 In addition to heightening the risk of vascular thrombosis, antiphospholipid antibodies increase vascular tone, thereby increasing the susceptibility to atherosclerosis, fetal loss, and neurological damage.6 A case-control study of 2,000 patients found a substantial increase in the risk of myocardial infarction associated with the presence of antiphospholipid antibodies (adjusted odds ratio of 1.8, 95 percent CI 1.2 to 2.6).7 A study of 27 patients with APS and 81 healthy control patients was undertaken to determine the prevalence of silent myocardial disease in patients with APS, using late gadolinium enhancement (LGE) of cardiac magnetic resonance imaging (CMRI). Myocardial ischemic disease, as characterized by LGE on CMRI, was present in 8 (29.6%) of 27 patients with APS, compared to 3 (3.5%) of the 81 healthy patients. Although both patients with APS and control subjects shared a low risk of cardiovascular events, as calculated with the Framingham risk equation (mean ± SD 5.1 ± 8.2% and 6.5 ± 7.6%, respectively, for the absolute risk within the next 10 years; P = 0.932), the prevalence of myocardial ischemia was more than 7 times higher in patients with APS (P = 0.0006 versus controls).8
For acute thrombotic events in patients with antiphospholipid antibodies, the first therapy is heparin, followed by warfarin until the INR is within the therapeutic range for two consecutive days.9 Warfarin is the standard of care for the chronic management of patients with APS. The current standard of care, developed through randomized controlled trials, is to maintain the INR between 2.0 and 3.0.10 In retrospective series, aspirin has been of minimal or no benefit for the prevention of thrombotic APS manifestations in patients who have experienced previous events.11 However, aspirin may be beneficial for prophylaxis in patients with antiphospholipid antibodies who do not have a history of thrombosis.12 Clopidogrel has been reported to be useful in at least one case report and is recommended by some experts.13 It may have a role in the treatment of APS, and in the primary and secondary prophylaxis in individuals who are allergic to aspirin. Statin treatment may also be an additional tool in treatment. Statins may influence endothelial activation of the anti-ß2GPI-induced proadhesive and proinflammatory endothelial phenotype, which may play a role in thrombosis.14 An expert panel convened to review the issue of cardiac disorders associated with APS suggested that hydroxychloroquine could be considered for cardiac protection.15 Data from animal models and limited, indirect evidence from studies in humans suggest that hydroxychloroquine reduces the size and persistence of venous thrombi16 and reverses platelet activation induced by immunoglobulin G (IgG) antiphospholipid antibodies.17 In a cross-sectional study designed to analyze risk factors for the APS, 77 APS patients with thrombotic events and 56 asymptomatic antiphospholipid antibody-positive patients were evaluated.12 In both univariate and multivariate analyses, hydroxychloroquine use was associated with a lack of thrombotic events. The optimal duration of anticoagulation for thromboembolic disease following a first event is uncertain in patients with APS. Lifelong therapy is prudent for many patients, especially with recurrence. The authors of a 2006 systematic review concluded that anticoagulation is warranted for an indefinite period for patients with APS and thrombosis.18 Low-dose aspirin is warranted if warfarin therapy must be discontinued.
We present herein a case of recurrent stent thrombosis in a patient with APS, managed successfully with serial revascularization procedures supported by dual antiplatelet therapy and warfarin.
The authors may be contacted via Dr. Jon George at: georgej@deborah.org
References
- Wilson WA, Gharavi AE, Koike T, et al. International consensus statement on preliminary classification criteria for definite antiphospholipid syndrome: report of an international workshop. Arthritis Rheum 1999; 42: 1309.
- Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006; 4: 295.
- Giannakopoulos B, Passam F, Ioannou Y, Krilis SA. How we diagnose the antiphospholipid syndrome. Blood 2009; 113: 985.
- Asherson RA, Khamashta MA, Ordi-Ros J, et al. The “primary” antiphospholipid syndrome: major clinical and serological features. Medicine (Baltimore) 1989; 68: 366.
- Bermas BL, et al. Pathogenesis of the antiphospholipid syndrome. Available online at https://www.uptodate.com/home/index.html. Accessed July 20, 2012.
- Mackworth-Young CG. Antiphospholipid syndrome: multiple mechanisms. Clin Exp Immunol 2004; 136: 393.
- Brey RL, Abbott RD, Curb JD, et al. beta(2)-Glycoprotein 1-dependent anticardiolipin antibodies and risk of ischemic stroke and myocardial infarction: the Honolulu heart program. Stroke 2001; 32: 1701.
- Sacré K, Brihaye B, Hyafil F, et al. Asymptomatic myocardial ischemic disease in antiphospholipid syndrome: a controlled cardiac magnetic resonance imaging study. Arthritis Rheum 2010; 62: 2093.
- Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126: 204S.
- Crowther MA, Ginsberg JS, Julian J, et al. A comparison of two intensities of warfarin for the prevention of recurrent thrombosis in patients with the antiphospholipid antibody syndrome. N Engl J Med 2003; 349: 1133.
- Rosove MH, Brewer PM. Antiphospholipid thrombosis: clinical course after the first thrombotic event in 70 patients. Ann Intern Med 1992; 117: 303.
- Erkan D, Yazici Y, Peterson MG, et al. A cross-sectional study of clinical thrombotic risk factors and preventive treatments in antiphospholipid syndrome. Rheumatology (Oxford) 2002; 41: 924.
- Bick RL. Antiphospholipid thrombosis syndromes. Clin Appl Thromb Hemost 2001; 7:241.
- Meroni PL, Raschi E, Testoni C et al. Statins prevent endothelial cell activation induced by antiphospholipid (anti-beta2-glycoprotein I) antibodies: effect on the proadhesive and proinflammatory phenotype. Arthritis Rheum 2001; 44: 2870-2878.
- Lockshin M, Tenedios F, Petri M, et al. Cardiac disease in the antiphospholipid syndrome: recommendations for treatment. Committee consensus report. Lupus 2003; 12: 518.
- Edwards MH, Pierangeli S, Liu X, et al. Hydroxychloroquine reverses thrombogenic properties of antiphospholipid antibodies in mice. Circulation 1997; 96: 4380.
- Espinola RG, Pierangeli SS, Gharavi AE, et al. Hydroxychloroquine reverses platelet activation induced by human IgG antiphospholipid antibodies. Thromb Haemost 2002; 87: 518.
- Erkan D, Leibowitz E, Berman J, Lockshin MD. Perioperative medical management of antiphospholipid syndrome: hospital for special surgery experience, review of literature, and recommendations. J Rheumatol 2002; 29: 843.
Disclosure: Dr. Hakimi reports no conflicts of interest regarding the content herein. Dr. Kovach reports he is a consultant for Spectranetics. Dr. George reports he is a consultant for Boston Scientific.
