


Prevention of Contrast-Induced Nephropathy: Clinical and Ethical Imperatives
Nurses play a vital role in assessing for and preventing the increased morbidity associated with contrast-induced nephropathy (CIN), an adverse outcome associated with studies requiring contrast medium. CIN is defined as an increase in baseline creatinine level by 25% or greater within 48 hours after a procedure requiring contrast material.1 Almost 10% of all hospital-acquired instances of renal insufficiency are directly attributed to studies that require contrast material.1 Patients in whom CIN develops after coronary angioplasty have an increased risk for death or myocardial infarction for as long as 5 years post procedure, and their in-hospital mortality rate exceeds 20%.1-2 As life expectancy and technological advances increase, a greater number of patients will likely undergo procedures such as computed tomography, arteriogram, pacemaker implantation, and cardiac catheterization, all of which involve the injection of contrast medium. Measures to avoid CIN should be undertaken in all cath labs.
Historically, a standardized protocol for screening, monitoring and prevention of CIN has not been used at our institution. Physicians reviewed the history and physical, and communicated a plan of care to the team for each individual patient. Diabetic patients receiving metformin therapy were routinely given a prescription for a follow-up basic metabolic panel (BMP) 48-72 hours following a cardiac cath procedure.
A clinical nurse looked into reducing the variety of contrast kept in the cath lab inventory. His experience sparked a greater curiosity and an increased desire to prevent CIN, leading to a literature review and a solicitation of expert opinions. As results were shared with cath lab staff at our facility, they exhibited a heightened awareness regarding the importance of risk screening prior to the procedure, monitoring for the amount of contrast medium given during the procedure, and the need for ongoing monitoring. Awareness was also enhanced regarding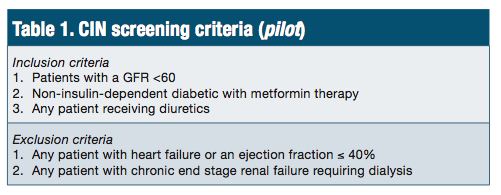 optimal hydration, long considered the gold standard in CIN prevention. Fluids dilute contrast medium, thereby decreasing direct nephrotoxic effects of inflammation and necrosis on renal cells.1
optimal hydration, long considered the gold standard in CIN prevention. Fluids dilute contrast medium, thereby decreasing direct nephrotoxic effects of inflammation and necrosis on renal cells.1
Ultimately, a team was formed, consisting of cath lab staff, physicians, and a clinical nurse specialist, to examine existing practices and design a pilot to integrate existing evidence.3 Pilot development is presently ongoing and the drafted pilot includes an initial CIN screening process, comprised of inclusion and exclusion criteria to assist in identifying patients at risk of CIN (Table 1). Targeted interventions for those at risk were derived from the existing evidence (Table 2).
Are there ethical implications?
Alongside the examination of clinical evidence, the authors also considered the ethical implications of not adopting existing evidence to prevent CIN. Although there are various hydration protocols in existing evidence, a common recommendation is 1 liter of normal saline solution infused starting 3 hours pre procedure and continuing for 6 to 8 hours post procedure.
implications of not adopting existing evidence to prevent CIN. Although there are various hydration protocols in existing evidence, a common recommendation is 1 liter of normal saline solution infused starting 3 hours pre procedure and continuing for 6 to 8 hours post procedure.
Not all patients that intersect with the cardiac catheterization lab can feasibly receive fluid administration of the recommended duration (e.g., scheduled outpatients), thus potentially creating an ethical dilemma. Even with knowledge of best practices, environmental barriers might result in inadvertent unethical practices for some populations, resulting in less than optimal outcomes. A short-term need for a procedure that requires contrast medium may have a long-term adverse effect on the patient’s renal function. While adequate hydration is associated with a reduction in the effects of contrast medium on renal function, care delivered over a long enough period of time to ensure that the total volume of fluid has been administered may be challenging due to time constraints, which could have inadvertent long-term implications. The cath lab CIN team at our institution decided to address this issue in part through attention to patient scheduling (Table 2).
What should be done?
As interventional studies become more common, nurses are poised to assess for risk factors and plan prophylaxis with physicians and pharmacists. Consideration must be given to determining a patient’s baseline serum creatinine level and kidney function, and his or her hydration state, as well as assessing any nephrotoxic medications that might need to be changed.1 In an effort to reduce the long-term effects of CIN, a standardized approach and adequate hydration, both pre and post procedure, is expected to be beneficial. By proactively designing a plan of care in association with existing evidence, cath lab staff can act in an ethical manner and assist in averting the potential adverse effects of CIN.
Conclusion
Deliberate measures to implement a structure and processes to produce optimal outcomes for those receiving contrast medium, regardless of existing barriers, is an ideal approach. Avoidance of CIN by an integration of the available evidence will place the care team in a position to avoid inadvertent unethical practices.
The authors can be contacted via Patricia Heffner MBA, BSN, RN, CEN, at patricia.heffner@myemail.indwes.edu.
References
- Isaac S. Contrast-induced nephropathy: nursing implications. Crit Care Nurse. 2012 Jun; 32(3): 41-48. doi: 10.4037/ccn2012516.
- Solomon RJ, Mehran R, Natarajan MK, Doucet S, Katholi RE, Staniloae CS, et al. Contrast-induced nephropathy and long-term adverse events: cause and effect? Clin J Am Soc Nephrol. 2009 Jul; 4(7): 1162-1169. doi: 10.2215/CJN.00550109.
- Titler MG, Kleiber C, Steelman VJ, Rakel BA, Budreau G, Everett LQ, et al. The Iowa model of evidence-based practice to promote quality care. Crit Care Nurs Clin North Am. 2001 Dec; 13(4): 497-509.
