


Persistent Left Superior Vena Cava
Abstract
A persistent left superior vena cava is a rare but most common thoracic vein anomaly. It is found in 0.3-0.5% of the general population, and in up to 12% in association with congenital heart diseases. An 81-year-old woman with history of paroxysmal atrial fibrillation and hypertension presented with palpitations and shortness of breath. Due to recurrent symptomatic bradycardias, pauses and asystole preceded by transient episodes of non-sustained ventricular tachycardia, she was referred for a permanent pacemaker placement. During cannulation of left cephalic vein for insertion of the permanent pacemaker leads, a persistent left superior vena cava was incidentally identified. To position the atrial lead optimally, the pacemaker was inserted from the right subclavian vein. Lack of knowledge of a persistent left superior vena cava can bring serious, adverse complications, if the team does not become aware of it in a timely fashion.
Introduction
A persistent left superior vena cava is a rare accessory thoracic vein from embryological life that can be present with or without a right superior vena cava. In general, a persistent left superior vena cava is incidentally identified during intra-thoracic procedures. However, co-morbid conditions such as congenital heart diseases, cardiac arrhythmias, or coronary sinus atresia can be present along with a persistent left superior vena cava.
Case report
An 81-year-old woman with past history of paroxysmal atrial fibrillation and hypertension presented with progressive shortness of breath. She was admitted for acute exacerbation of congestive heart failure due to systolic dysfunction, requiring diuretic administration. She had several episodes of severe sinus bradycardia with asystole and several pauses of up to 4 seconds during hospitalization. There were also several runs of non-sustained ventricular tachycardia, immediately preceding the sinus bradycardia episodes. Her echocardiogram was suboptimal due to poor acoustics window, which showed a limited left ventricular (LV) function assessment.
After the patient was medically stabilized, a nuclear SPECT stress image showed moderate, reversible ischemia involving the inferior wall, extending into small area of left ventricular apex, and her left ventricular ejection fraction (LVEF) was reported as 37%. Due to a substantial limitation in LVEF measurement, a multi-gated acquisition (MUGA) scan was obtained for a more accurate assessment of her left ventricular function and to assess any need for implantable cardioverter defibrillator (ICD) placement. The MUGA scan revealed a normal resting left and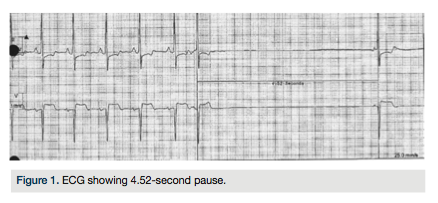 right ventricular function with a calculated LVEF of 58%, and confirmed ICD placement was not necessary.
right ventricular function with a calculated LVEF of 58%, and confirmed ICD placement was not necessary.
During cardiac rhythm monitoring, several episodes of severe sinus bradycardia occurred, with a few transient asystole and sinus pauses of up to 4 seconds (Figure 1). The patient also had several runs of non-sustained ventricular tachycardia (Figure 2), usually immediately preceded by the sinus bradycardia episodes. Management of ventricular tachyarrhythmias with beta-blockers was limited due to concomitant episodes of sinus bradycardia. It was decided to insert a permanent pacemaker,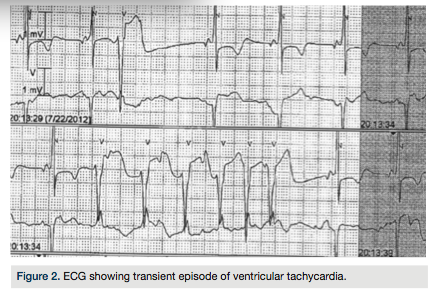 which would permit the safe administration of beta blockers to treat her symptomatic runs of non-sustained ventricular tachyarrhythmias and paroxysmal atrial tachyarrhythmias.
which would permit the safe administration of beta blockers to treat her symptomatic runs of non-sustained ventricular tachyarrhythmias and paroxysmal atrial tachyarrhythmias.
Under fluoroscopic guidance, a left cephalic vein approach was used to gain access to the transvenous route of the heart chambers. While inserting the guide wire, the left subclavian vein had an unusual course, and the guide wire crossed medially behind the heart, suggesting the presence of a persistent left superior vena cava, which was then confirmed by venography (Figure 3). Although a right ventricular pacing lead could still be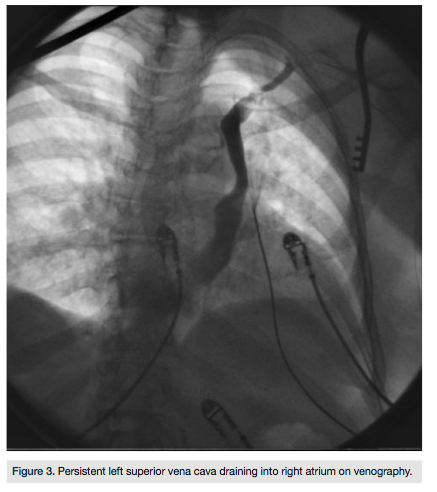 placed, an atrial lead could not be positioned superiorly in an optimal position via this approach. The left cephalic vein approach was abandoned and the pacemaker was successfully inserted via the right pectoral approach through the right cephalic vein (Figure 4).
placed, an atrial lead could not be positioned superiorly in an optimal position via this approach. The left cephalic vein approach was abandoned and the pacemaker was successfully inserted via the right pectoral approach through the right cephalic vein (Figure 4).
Discussion
A persistent left superior vena cava is a rare thoracic vein anomaly, but it is the most commonly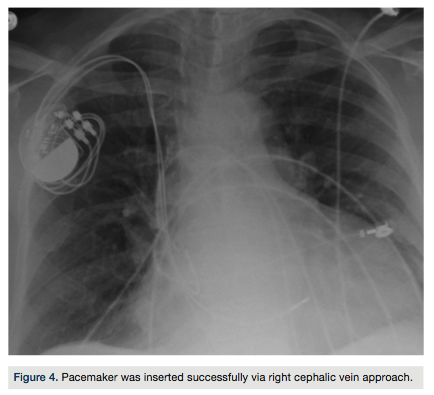 reported accessory thoracic vein. The anatomical course of a persistent left superior vena cava runs along the aortic arch laterally, passes anterior to the hilum, enters the pericardium from the posterior atrioventricular groove, and ultimately, drains into the coronary sinus1-3 in over 90% of cases. In less than 10%, it connects into the left atrium. In the latter case, a right-to-left shunt ensues, with venous blood from left side of the head and neck draining into the left atrium. Although cyanosis might not be observed, as the mixed amount of arterial and venous blood is minimal4, risk for systemic embolization may exist. When a persistent left superior vena cava drains into the coronary sinus, it can cause dilatation of the coronary sinus and partially occlude the mitral valve, impairing the left ventricular inflow, with risk for thrombus formation.5,6
reported accessory thoracic vein. The anatomical course of a persistent left superior vena cava runs along the aortic arch laterally, passes anterior to the hilum, enters the pericardium from the posterior atrioventricular groove, and ultimately, drains into the coronary sinus1-3 in over 90% of cases. In less than 10%, it connects into the left atrium. In the latter case, a right-to-left shunt ensues, with venous blood from left side of the head and neck draining into the left atrium. Although cyanosis might not be observed, as the mixed amount of arterial and venous blood is minimal4, risk for systemic embolization may exist. When a persistent left superior vena cava drains into the coronary sinus, it can cause dilatation of the coronary sinus and partially occlude the mitral valve, impairing the left ventricular inflow, with risk for thrombus formation.5,6
Patients with a persistent left superior vena cava may develop various forms of cardiac arrhythmias such as sinus node and atrioventricular node dysfunctions, resulting from enlargement of the right atrium or dilation of the coronary sinus. Furthermore, automatic “pacemaker” activities may be present in tissues located at the junction of sinus venosus and common cardinal vein in the embryo heart.7 Normally, the sinoatrial node serves as the sole pacemaker in healthy adults. However, in patients with a persistent left common cardinal vein, ectopic pacemaker activities can be present at the junction of sinus venosus and left common cardinal vein, causing an aberrant conduction system with arrhythmias.7,8
A persistent left superior vena cava is usually incidentally found during central venous cannulation, pacemaker insertion, ICD implantation, cardiopulmonary bypass, or autopsy. Therefore, in central line placement in patients with a left superior vena cava, it is prudent not to irritate the coronary sinus, as severe hypotension, arrhythmias, myocardial ischemia, and even cardiac arrest may develop. In general, patients with a persistent left superior vena cava are asymptomatic, especially in the absence of co-morbid congenital abnormalities such as atrial septal defect, ventricular septal defect, pulmonary stenosis, Tetralogy of Fallot, and anomalous pulmonary drainage.4
Embryology of persistent left superior vena cava
Sinus venosus, from which the primitive sinoatrial node and coronary sinus develops, resides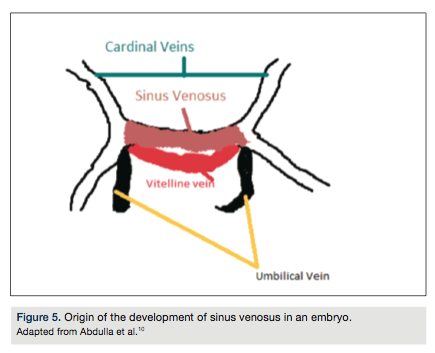 dorsally to the right atrium. In a fifth-week fetus, the common cardinal veins, the umbilical vein, and the vitelline vein drain into the sinus venosus (Figure 5). The common cardinal vein serves as the major venous drainage of the embryo, with the anterior cardinal vein carrying blood from the cephalic part of the embryo, while the posterior cardinal vein carries blood from the caudal part of the embryo. The vitelline vein connects with the yolk sac to the sinus venosus. Umbilical veins are the sources for carrying oxygenated blood from the placenta for the embryo.9 The distal part of the left cardinal vein then degenerates and the proximal portion connects to the right anterior cardinal vein, forming the superior vena cava. The left posterior cardinal vein degenerates with the formation of ligament of Marshall (Figure 6), a process completed around the eighth week of embryo life.10 The failure of the left posterior cardinal vein to degenerate results in a persistent left superior vena cava state, even in association with a left
dorsally to the right atrium. In a fifth-week fetus, the common cardinal veins, the umbilical vein, and the vitelline vein drain into the sinus venosus (Figure 5). The common cardinal vein serves as the major venous drainage of the embryo, with the anterior cardinal vein carrying blood from the cephalic part of the embryo, while the posterior cardinal vein carries blood from the caudal part of the embryo. The vitelline vein connects with the yolk sac to the sinus venosus. Umbilical veins are the sources for carrying oxygenated blood from the placenta for the embryo.9 The distal part of the left cardinal vein then degenerates and the proximal portion connects to the right anterior cardinal vein, forming the superior vena cava. The left posterior cardinal vein degenerates with the formation of ligament of Marshall (Figure 6), a process completed around the eighth week of embryo life.10 The failure of the left posterior cardinal vein to degenerate results in a persistent left superior vena cava state, even in association with a left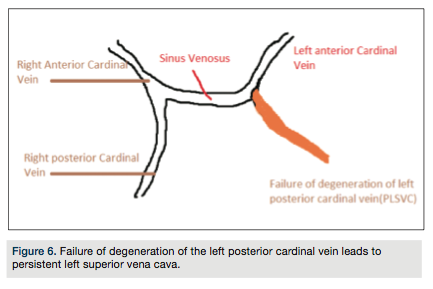 azygos vein on some occasions.11
azygos vein on some occasions.11
Conclusion
A persistent left superior vena cava should be considered when experiencing difficulties with central venous access, since it is one of the most common thoracic anomalies. It is important to notice and recall abnormalities of the anatomic structures that could be accidentally discovered during thoracic operations or accessing central lines. Venography, computed tomography angiography and cardiovascular magnetic resonance imaging may be helpful to identify a persistent left superior vena cava if in doubt and to avoid unfavorable results.
This article received a double-blind peer review from members of the Cath Lab Digest editorial board.
The authors may be contacted via Dr. Koroush Khalighi at koroushkhalighi@gmail.com.
References
- Cormier MG, Yedlicka JW, Gray RJ, et al. Congenital anomalies of the superior vena cava: a CT study. Semin Roentgenol. 1989 Apr; 24(2): 77-83.
- Gaynor JW, Weinberg PM, Spray TL. Congenital heart surgery nomenclature and database project: systemic venous anomalies. Ann Thorac Surg. 2000 Apr; 69(4 Suppl): S70-S76.
- Sarodia BD, Stoller JK. Persistent left superior vena cava: case report and literature review. Respir Care. 2000 Apr; 45(4): 411-416.
- MacDonald ST, Emmanuel Y, Myerson S, Prendergast B, Neubauer S, Leeson P. Absent right superior vena cava: multimodality imaging of upper body venous drainage via left-sided superior vena cava and azygos venous system. Circ Cardiovasc Imaging. 2009 Sep; 2(5): e34-e36.
- Muster AJ, Naheed ZJ, Backer CL, Mavroudis C. Is surgical ligation of an accessory left superior vena cava always safe? Pediatr Cardiol. 1998 Jul-Aug; 19(4): 352-354.
- Santoscoy R, Walters HL 3rd, Ross RD, Lyons JM, Hakimi M. Coronary sinus ostial atresia with persistent left superior vena cava. Ann Thorac Surg. 1996 Mar; 61(3): 879-882.
- Pachon M JC, Pachon M EI, Pachon M JC, Lobo TJ, Pachon MZ, Vargas RN, et al. A new treatment for atrial fibrillation based on spectral analysis to guide the catheter RF-ablation. Europace. 2004 Nov; 6(6): 590-601.
- Hsu LF, Jaïs P, Keane D, Wharton JM, Deisenhofer I, Hocini M, et al. Atrial fibrillation originating from persistent left superior vena cava. Circulation. 2004 Feb 24; 109(7): 828-832.
- Paval J, Nayak S. A persistent left superior vena cava. Singapore Med J. 2007 Mar; 48(3): e90-e93.
- Abdulla R, Blew GA, Holterman MJ. Cardiovascular embryology. Pediatr Cardiol. 2004 May-Jun; 25(3): 191-200.
- Uemura M, Takemura A, Ehara D, Yasumitsu H, Ohnishi Y, Suwa F. Left superior vena cava with left azygos vein. Okajimas Folia Anat Jpn. 2009 Aug; 86(2): 55-60.
