


Percutaneous Paravalvular Leak Closure in the Aortic Position
Case 1
 An 83-year-old male, with history of a bioprosthetic aortic valve replacement (Medtronic Mosaic #25) and coronary artery bypass grafting approximately eight months earlier, presented with severe shortness of breath secondary to acute decompensated heart failure. Transthoracic echocardiography demonstrated a moderately diminished left ventricular ejection fraction of 30-40% with a well-seated bioprosthetic aortic valve and severe paravalvular aortic regurgitation. The patient was subsequently referred for further evaluation and percutaneous closure of paravalvular aortic regurgitation.
An 83-year-old male, with history of a bioprosthetic aortic valve replacement (Medtronic Mosaic #25) and coronary artery bypass grafting approximately eight months earlier, presented with severe shortness of breath secondary to acute decompensated heart failure. Transthoracic echocardiography demonstrated a moderately diminished left ventricular ejection fraction of 30-40% with a well-seated bioprosthetic aortic valve and severe paravalvular aortic regurgitation. The patient was subsequently referred for further evaluation and percutaneous closure of paravalvular aortic regurgitation.
 The patient underwent general anesthesia and endotracheal intubation for transesophageal echocardiography (TEE) evaluation in the cardiac catheterization laboratory. TEE confirmed moderate to severe paravalvular regurgitation adjacent to the valve within the non-coronary cusp (Figure 1). A 6 French multipurpose guide catheter (Launcher, Medtronic) was positioned within the aortic root and a Glidewire (Terumo Medical) advanced through the paravalvular leak under fluoroscopic and transesophageal guidance. The soft
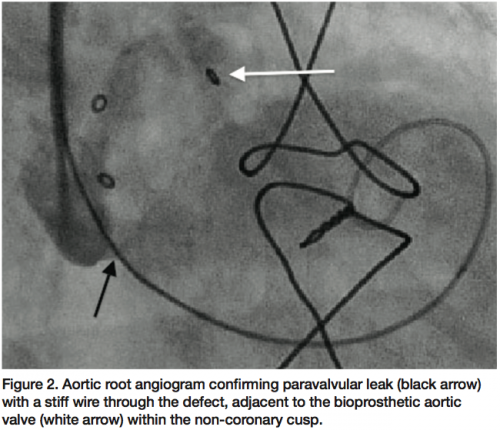
The patient underwent general anesthesia and endotracheal intubation for transesophageal echocardiography (TEE) evaluation in the cardiac catheterization laboratory. TEE confirmed moderate to severe paravalvular regurgitation adjacent to the valve within the non-coronary cusp (Figure 1). A 6 French multipurpose guide catheter (Launcher, Medtronic) was positioned within the aortic root and a Glidewire (Terumo Medical) advanced through the paravalvular leak under fluoroscopic and transesophageal guidance. The soft 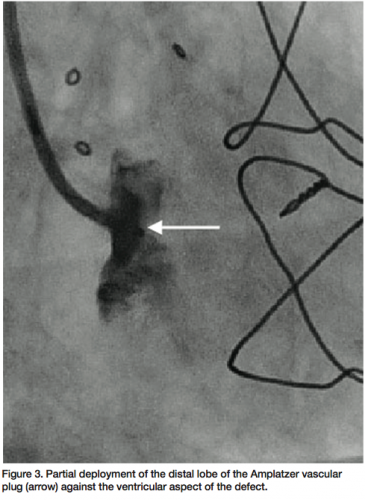 Glidewire was exchanged for an Amplatz stiff wire (Cook Medical) and a 6 French 90 cm Pinnacle sheath (Terumo Medical) advanced over the Amplatz stiff wire through the paravalvular defect into the left ventricle (Figure 2). The stiff wire was removed and a 10 mm Amplatzer vascular plug II (AGA Medical) advanced through the sheath. The distal lobe of the device was deployed on the ventricular side and withdrawn to pull against the ventricular aspect of the
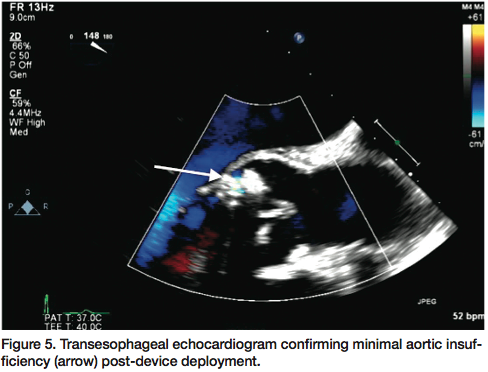
Glidewire was exchanged for an Amplatz stiff wire (Cook Medical) and a 6 French 90 cm Pinnacle sheath (Terumo Medical) advanced over the Amplatz stiff wire through the paravalvular defect into the left ventricle (Figure 2). The stiff wire was removed and a 10 mm Amplatzer vascular plug II (AGA Medical) advanced through the sheath. The distal lobe of the device was deployed on the ventricular side and withdrawn to pull against the ventricular aspect of the 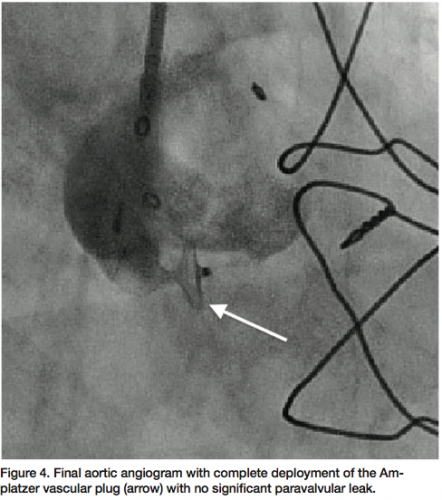 defect (Figure 3). The two proximal lobes of the device were then packed against the aortic side of the defect and with adequate positioning confirmed, the delivery system disengaged and final angiographic (Figure 4) and transesophageal images obtained, demonstrating no significant aortic insufficiency (Figure 5). All catheters and sheaths were removed, with hemostasis achieved using a vascular closure device. The patient was discharged home the following day without any complications.
defect (Figure 3). The two proximal lobes of the device were then packed against the aortic side of the defect and with adequate positioning confirmed, the delivery system disengaged and final angiographic (Figure 4) and transesophageal images obtained, demonstrating no significant aortic insufficiency (Figure 5). All catheters and sheaths were removed, with hemostasis achieved using a vascular closure device. The patient was discharged home the following day without any complications.
Case 2
A 56-year-old male status post bioprosthetic aortic valve replacement (20 mm Edwards Lifesciences) approximately six months earlier, presented with progressive decompensated heart failure (New York Heart Association Class III, Killip Class II). Transthoracic echocardiogram demonstrated a bioprosthetic aortic valve with moderate paravalvular regurgitation, in addition to mild central 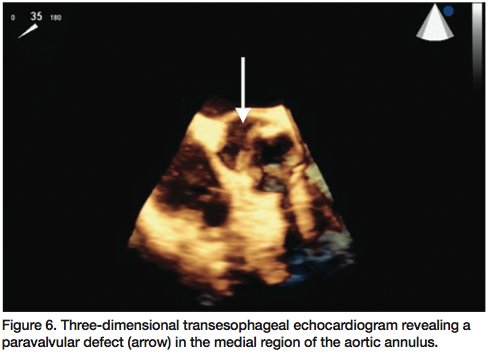 aortic insufficiency with preserved left ventricular ejection fraction of 50-55%. Three-dimensional transesophageal echocardiogram confirmed 3+ paravalvular aortic regurgitation originating from the medial region of the aortic annulus (Figure 6). The patient was then referred for percutaneous closure due to high associated mortality risk of redo sternotomy.
aortic insufficiency with preserved left ventricular ejection fraction of 50-55%. Three-dimensional transesophageal echocardiogram confirmed 3+ paravalvular aortic regurgitation originating from the medial region of the aortic annulus (Figure 6). The patient was then referred for percutaneous closure due to high associated mortality risk of redo sternotomy.
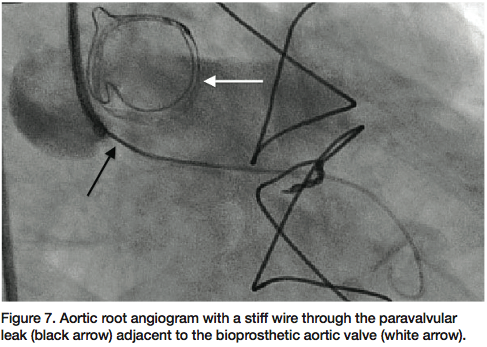 The patient underwent general anesthesia and endotracheal intubation for TEE evaluation in the cardiac catheterization laboratory. The paravalvular leak was crossed using a 6 French multipurpose diagnostic catheter and angled Glidewire, followed by a 6 French shuttle sheath (Cook Medical) over an Amplatz stiff wire (Figure 7). Using TEE and fluoroscopy, an 8 mm Amplatzer vascular plug II (AGA Medical) was deployed successfully, with persistent moderate regurgitation from the anteromedial region of the paravalvular aortic leak (Figure 8). The defect was
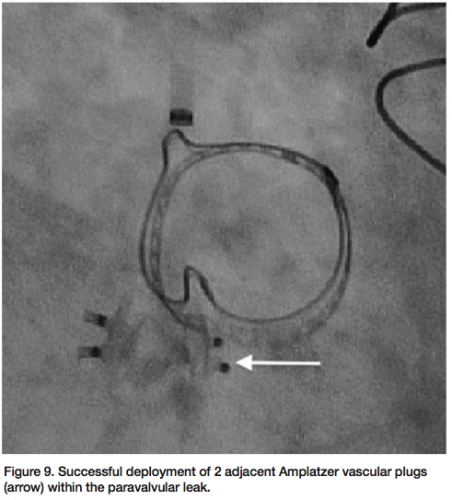
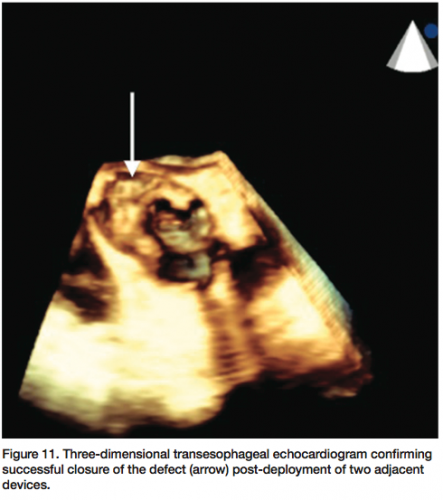
The patient underwent general anesthesia and endotracheal intubation for TEE evaluation in the cardiac catheterization laboratory. The paravalvular leak was crossed using a 6 French multipurpose diagnostic catheter and angled Glidewire, followed by a 6 French shuttle sheath (Cook Medical) over an Amplatz stiff wire (Figure 7). Using TEE and fluoroscopy, an 8 mm Amplatzer vascular plug II (AGA Medical) was deployed successfully, with persistent moderate regurgitation from the anteromedial region of the paravalvular aortic leak (Figure 8). The defect was 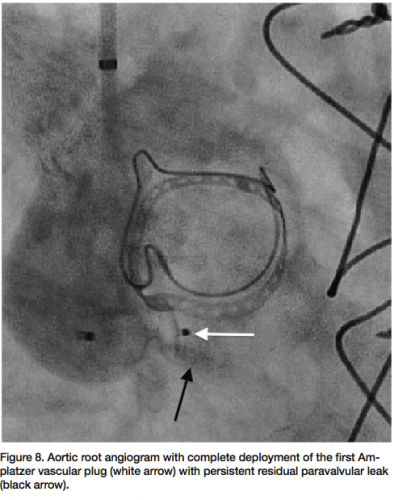 recrossed with a 5 French EBU guide catheter (Medtronic), followed by placement of a second 8 mm Amplatzer vascular plug (Figure 9). Final angiography (Figure 10) and TEE (Figure 11) of the paravalvular leak after two adjacent vascular plugs demonstrated no significant residual paravalvular leak. All catheters and sheaths were removed, with hemostasis achieved using a vascular closure device. The patient was discharged home without complications the following day.
recrossed with a 5 French EBU guide catheter (Medtronic), followed by placement of a second 8 mm Amplatzer vascular plug (Figure 9). Final angiography (Figure 10) and TEE (Figure 11) of the paravalvular leak after two adjacent vascular plugs demonstrated no significant residual paravalvular leak. All catheters and sheaths were removed, with hemostasis achieved using a vascular closure device. The patient was discharged home without complications the following day.
Discussion
 Paravalvular regurgitation is a known complication of valve replacement, with an incidence rate of 3 to 7%.1-6 This potential complication arises secondary to incomplete apposition of the sewing ring to the native tissue from suture dehiscence, which occurs more commonly in patients with heavy annular calcifications, localized infections, or related to surgical technique.2,7,8 Additionally, reoperation for repair of peravalvular regurgitation carries significantly increased procedural mortality of 6 to 15% and higher incidence of
Paravalvular regurgitation is a known complication of valve replacement, with an incidence rate of 3 to 7%.1-6 This potential complication arises secondary to incomplete apposition of the sewing ring to the native tissue from suture dehiscence, which occurs more commonly in patients with heavy annular calcifications, localized infections, or related to surgical technique.2,7,8 Additionally, reoperation for repair of peravalvular regurgitation carries significantly increased procedural mortality of 6 to 15% and higher incidence of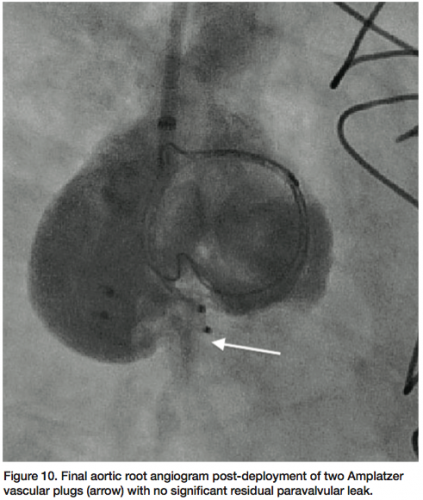 perioperative complications.7-10 Although a majority of patients are asymptomatic, with a small, coincidental paravalvular leak, severe paravalvular regurgitation can lead to significant morbidity, including heart failure, hemolytic anemia, pulmonary hypertension, and infective endocarditis.2,3,6 Consequently, percutaneous repair of paravalvular regurgitation has been identified as an alternative therapy, primarily to avoid the risks of open surgical correction.
perioperative complications.7-10 Although a majority of patients are asymptomatic, with a small, coincidental paravalvular leak, severe paravalvular regurgitation can lead to significant morbidity, including heart failure, hemolytic anemia, pulmonary hypertension, and infective endocarditis.2,3,6 Consequently, percutaneous repair of paravalvular regurgitation has been identified as an alternative therapy, primarily to avoid the risks of open surgical correction.
 A case series by Sorajja et al demonstrated safe and successful percutaneous repair of paravalvular prosthetic regurgitation in selected high-risk, symptomatic patients, resulting in significant clinical improvement without the need for open surgical correction.11 An additional case series of 10 patients by Pate et al demonstrated successful percutaneous closure when patients were not candidates for surgery, with 7 out of 10 achieving complete or partial occlusion, and 4 out of 10 requiring a second procedure.12 Herein, our cases likewise illustrate the use of a percutaneous approach for closure of paravalvular aortic leaks as an alternative strategy for redo surgery with excellent clinical outcomes.
A case series by Sorajja et al demonstrated safe and successful percutaneous repair of paravalvular prosthetic regurgitation in selected high-risk, symptomatic patients, resulting in significant clinical improvement without the need for open surgical correction.11 An additional case series of 10 patients by Pate et al demonstrated successful percutaneous closure when patients were not candidates for surgery, with 7 out of 10 achieving complete or partial occlusion, and 4 out of 10 requiring a second procedure.12 Herein, our cases likewise illustrate the use of a percutaneous approach for closure of paravalvular aortic leaks as an alternative strategy for redo surgery with excellent clinical outcomes.
The authors can be contacted via Dr. George at georgej@deborah.org.
This article received double-blind peer review from members of the Cath Lab Digest editorial board.
Disclosure: Dr. George reports he is a consultant for Boston Scientific. Dr. Trayer and Dr. Kovach report no conflicts of interest regarding the content herein.
References
- Akins CW. Results with mechanical cardiac valvular prostheses. Ann Thorac Surg 1995;60:1836-1844.
- Rallidis LS, Moyssakis IE, Ikonomidis I, Nihoyannopoulos P. Natural history of early aortic paraprosthetic regurgitation: A five-year follow-up. Am Heart J 1999;138:351-357.
- O’Rourke DJ, Palac RT, Malenka DJ, et al. Outcome of mild periprosthetic regurgitation detected by intraoperative transesophageal echocardiography. J Am Coll Cardiol 2001;38:163-166.
- Davila-Roman VG, Waggoner AD, Kennard ED, et al. Prevalence and severity perivalvular regurgitation in the artificial valve endocarditis reduction trial (AVERT) echocardiography study. J Am Coll Cardiol 2004;44:1467-1472.
- Murphy DR, Henry DS, Ellison LH, et al. Natural history of small periprosthetic regurgitation following prosthetic valve replacement. Circulation 1998;92(Suppl I):464.
- Movsowitz HD, Shah SI, Ioli A, Kotler MN, Jacobs LE. Long-term follow-up of mitral paraprosthetic regurgitation by transesophageal echocardiography. J Am Soc Echocardiogr 1994;7:488-492.
- Husebye DG, Pluth JR, Piehler JM, et al. Reoperation on prosthetic heart valves. J Thorac Cardiovasc Surg 1983;86:543-552.
- Miller DL, Morris JJ, Schaff HV, Mullany CJ, Nishimura RA, Orszulak TA. Reoperation for aortic periprosthetic leakage: Identification of patients at risk and results of operation. J Heart Valve Dis 1995:160-165.
- Akins CW, Bitondo JM, Hilgenberg AD, Vlahakes GJ, Madsen JC, MacGillivray TE. Early and late results of the surgical correction of cardiac prosthetic perivalvular leaks. J Heart Valve Dis 2005;14:792-800.
- De Cicco G, Russo C, Moreo AN, et al. Mitral valve periprosthetic leakage: Anatomical observations in 135 patients from a multicentre study. Eur J Cardiothorac Surg 2006;30:887-891.
- Sorajja P, Cabalka A, Hagler D, et al. Successful percutaneous repair of perivalvular prosthetic regurgitation. Catheter Cardiovasc Interv 2007;70:815-823.
