


Percutaneous Coronary Intervention without On-Site Open Heart Surgery: A “State of The Union” for 2013
 Hard to believe that it has been a little over three years since our article, “A ‘State of the Union’: Percutaneous Coronary Intervention (PCI) Without On-Site Open Heart Surgery,” appeared in Cath Lab Digest in May of 2009. Fortunately, much has improved across the country relative to access to life-saving PCI, and in fact, regulatory changes are still occurring across the country in response to the recent 2011 PCI guideline update1, even today!
Hard to believe that it has been a little over three years since our article, “A ‘State of the Union’: Percutaneous Coronary Intervention (PCI) Without On-Site Open Heart Surgery,” appeared in Cath Lab Digest in May of 2009. Fortunately, much has improved across the country relative to access to life-saving PCI, and in fact, regulatory changes are still occurring across the country in response to the recent 2011 PCI guideline update1, even today!
Published in November 2011, the PCI guidelines elevated the classification (from a Class III to a IIb indication) and level of evidence supporting elective PCI being performed in a hospital with open-heart surgery off-site (PCI with SOS). The societies have based their latest guidelines on the success and preliminary outcomes from the most recent national CPORT-E trial, and have considered other national studies such as a Mayo Clinic meta-analysis.
 Corazon has found that, in response to the 2011 published guidelines, many individual state regulating bodies have begun to revise, or are in discussions to consider, revisions to their current PCI regulations. This is not to say the process for offering PCI with SOS will be any less difficult for hospitals in those states, but perhaps having the medical professional societies as a champion to drive change within a particular region will provide the support necessary to impact change and ultimately save the lives of patients with acute myocardial infarction (MI). Also, the promotion of elective PCI with SOS within the latest guidelines can support the provision of more timely access to care to those patients requiring coronary ischemic management.
Corazon has found that, in response to the 2011 published guidelines, many individual state regulating bodies have begun to revise, or are in discussions to consider, revisions to their current PCI regulations. This is not to say the process for offering PCI with SOS will be any less difficult for hospitals in those states, but perhaps having the medical professional societies as a champion to drive change within a particular region will provide the support necessary to impact change and ultimately save the lives of patients with acute myocardial infarction (MI). Also, the promotion of elective PCI with SOS within the latest guidelines can support the provision of more timely access to care to those patients requiring coronary ischemic management.
Our experience across the United States continues to suggest a change in the perception and acceptance of PCI with SOS. Many of our clients interested in offering this service will first ask, is it feasible and/or reasonable to consider such an expansion? In addition to making the business case, several critical program components must be taken into consideration, such as physician commitment and expertise, staff training and competencies, emergency medical support, the ability to offer 24/7/365 access to the service for the acute MI patient population, and the creation of a formal tertiary relationship with an open-heart provider, just to name a few.
When truly considering these questions, many hospital administrators fully recognize the obstacles they may face, whether they are challenges from the state health department, opposition from cardiac full-continuum of care (inclusive of open-heart surgery) competitors, or even the lack of aforementioned critical program components. However, increasing immediate access to best-practice care delivery for heart attack victims could serve as the motivation for an official evaluation of program feasibility, followed by a strategic plan for the expansion.
Despite the limitations, growing support to allow elective PCI with off-site open heart surgical support is sweeping the United States due to outcomes data that clearly proves elective PCI is just as safe at the community provider with SOS compared to tertiary centers that provide on-site open heart surgery. Of course, for the acute MI patient population, we cannot understate the evidence of primary PCI being first choice of treatment and superior to thrombolytic therapy.
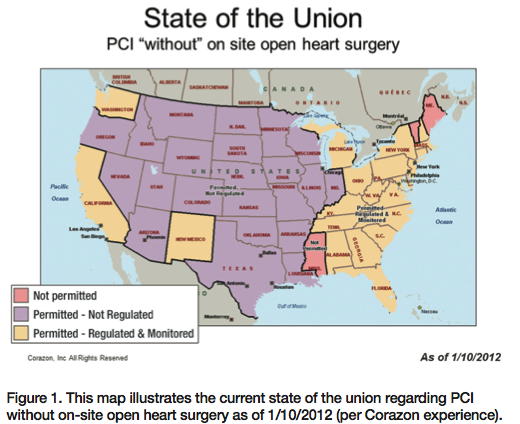
Corazon closely tracks the state activity of PCI with SOS. Listed below are several states that have endorsed varying levels of practice and in some cases, have begun to take the necessary, although daunting, steps to affect change within their state. Let’s look across the country, and more specifically at the east coast, recognizing that PCI continues to remain a hotbed of activity (Figure 1).
For several years, New Jersey has permitted hospitals without on-site open-heart surgery to offer primary PCI, though only 12 hospitals have been granted permission to offer elective PCI with SOS, under the auspice of CPORT-E trial participation. Recently, several New Jersey hospitals have developed a consortium to engage the New Jersey Department of Health to create revisions that will allow hospitals without on-site open-heart surgery to provide elective PCI without having to participate in a national registry, and without limiting the “number” of elective PCI providers. Although New Jersey has taken on this daunting task, it may take several months or even years, for the State to come to a consensus allowing elective PCI with SOS to be offered beyond those facilities currently providing services.
Pennsylvania is a non-certificate of need (CON) state. This allows those hospitals wanting to expand into additional and often more advanced cardiovascular services such as open-heart surgery, to do so without a formal CON application that usually demonstrates services based on particular need. As is common in many non-CON states, Pennsylvania does have prohibitory department of health (DOH) codes limiting PCI with SOS. In 2001, the Commonwealth of Pennsylvania was approached by many community providers asking to offer PCI at their facilities with SOS. After many meetings with officials at the Commonwealth DOH and the engagement of legal support, ten programs were permitted to initiate PCI as part of a demonstration project to offer both emergent and elective PCI. There were specific criteria that each selected facility was required to meet, and specific quality metrics that were collected and reported to the Commonwealth as part of an independent settlement agreement specific to each organization. In essence, the Commonwealth was granting ‘exceptions’ to the codes and no two agreements were the same. It has been almost 12 years since these programs began offering PCI services and thousands of successful outcomes have been recorded. One must ask, “Has the burden been met?” In 2008, the Commonwealth was once again challenged by additional providers wanting to offer elective PCI with SOS. It responded by permitting those facilities to commence services. However, in this particular subgroup, the facilities agreed to participate in the CPORT-E study, and do so at their own expense. Recently, approximately six of these providers have initiated discussions with the Department of Health to develop a standard for those currently offering PCI, both PCI with surgery on-site and off-site, as well for those hospitals considering expanding acute MI services to include elective PCI. The Pennsylvania DOH does recognize the recent changes published by the professional societies. The DOH will be working over the next several months with those hospitals to assure that standard care practices and quality review processes are developed and maintained moving forward.
South Carolina has also recognized the revised 2011 PCI guidelines and is proposing the adoption of those guidelines into their existing State Health Plan, and in fact, presented the proposed changes to the States Health Plan in November 2012.
Alabama has also proposed written changes encompassing the same 2011 guidelines, and has extrapolated physician and quality criteria directly from the guidelines that must be met in order to provide this life-saving service. The state has recently reported that the new language, which is now posted for public comment, is available for review and comment through January 2013.
The Maryland Healthcare Commission continues to debate whether or not to lift certain geographic restrictions, as well address the recent PCI guidelines that would allow other community-based providers without SOS to expand their services beyond primary or emergent PCI.
Over this past year, Kentucky has drafted criteria and is awaiting a decision by the State that will formally recognize and adopt these criteria into their current State Health Plan. A decision was made to “maintain the current status” in November of 2012.
We continue to recognize those states, such as Georgia and Florida, that have risen above bureaucracy and stalemate politics, and have allowed community-based hospitals to expand cardiovascular services beyond diagnostic services only. In these states, even emergent PCI with expansion to elective PCI with SOS services is being developed in many communities. In Georgia, Corazon continues to act as a “third-party verifier,” and at the request of the hospital, our team will provide an annual quality review to ensure PCI providers continue to meet necessary program requirements, and in many cases, excel in quality outcomes. Our team often receives information about the number lives saved due to those programs’ ability to offer life-saving PCI service.
Most states in the center of the country have little to no restrictions governing PCI at a facility without on-site open-heart surgery, and this has not changed. However, there are exceptions to this rule.
In 2009, California, a non-CON state, addressed elective PCI without SOS by allowing up to six hospitals that met defined state requirements to participate in an ongoing pilot project. Those facilities approved to offer elective PCI had to meet the CDPH (California Department of Public Health) written requirements/criteria.In addition, the hospitals had to submit an application to be considered and selected to participate within the pilot program. The CDPH will look at all aspects of the pilot programs from costs, safety, and quality outcomes. In addition, the department (at their discretion) has indicated that it may charge the pilot facilities a fee for oversight, should it be deemed necessary from a funding standpoint. The California pilot program end date is scheduled for January 2014, at which time, the CDPH will evaluate and determine the future of PCI with SOS in California. The Department will submit a written report 90 days after the completion of the pilot program, and then decide whether or not additional programs wanting to offer PCI without SOS will be permitted.
Although changes continue to occur across the United States regarding PCI without open-heart surgery on-site, we cannot understate the value of developing a solid plan for any program expansion. Careful planning and continued market surveillance, coupled with a savvy administration and collaboration among physicians, clinicians, and future partners is no doubt “mission critical” for a successful program expansion. We continue to recommend that any program looking to expand cardiovascular services to PCI submit to the American College of Cardiology (ACC)-National Cardiovascular Data Registry (NCDR) CathPCI Registry. Not only does participation in the Registry provide an organization with benchmarking opportunities, but it will continue to drive national recognition and quality excellence among other providers. In many of the states above, existing or proposed criteria includes mandatory participation in the ACC-NCDR National Registry.
As many community-based providers consider expansion to PCI with SOS, and given all of the recent literature supporting its safety and efficacy, we should perhaps no longer debate whether the burden has been met, but rather move forward, considering the positive impact of these changes to programs across the country, especially in terms of improved access to life-saving care for the patients who need it most.
Amy Newell is a Vice President at Corazon, Inc., focused on strategic program development for the heart, vascular, neuro, and orthopedic specialties, offering consulting, recruitment, interim management and physician practice & alignment services. To learn more, visit www.corazoninc.com or call (412) 364-8200. To reach Amy, email anewell@corazoninc.com.
Reference
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011 Dec 6;58(24):e44-122. doi: 10.1016/j.jacc.2011.08.007.
